Hemodialysis treatment
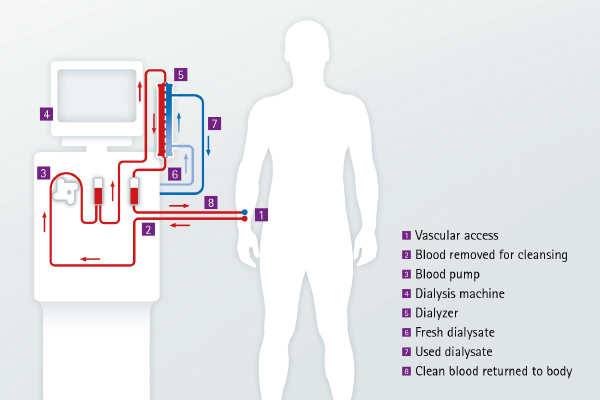
The process of hemodialysis cleans your blood using a special type of filter called a dialyzer. To perform this dialysis therapy relatively large quantities of blood must be handled in a relatively short period of time. The normal blood vessels are not suitable for handling this flow due to difficulties with accessibility or pressure levels that are too low. Therefore, a special vascular access point is established to support chronic dialysis treatment – a so-called AV (arteriovenous) fistula or shunt. A small surgical procedure is necessary to create this access point. The fistula heals within a few days, but it requires several weeks before it is ready for full use as a vascular access point. It is then simple to conduct the blood from the AV fistula to the dialyzer and back to the body again through special tubing also referred to as bloodlines.
During treatment, the blood is cleaned in the dialyzer. The cleaning process does not cause any pain and many patients will experience improvement of their condition especially in the beginning of dialysis treatment. However, if you feel unwell or uncomfortable during treatment, you should tell the staff, who will help you. Depending on your medical history, you will usually undergo hemodialysis three times a week with an average session time of 4-5 hours each treatment.
Hemodialysis is the most common method used to treat chronic kidney failure. It is mostly performed at a renal care center under the supervision of experienced and well-trained medical staff.
Advantages
- You are completely free on the days between dialysis sessions and need not worry about treatment.
- Thanks to modern technology, blood purification has become gentler and more effective.
- Treatment usually takes place in a renal care center.
Frequently asked questions: Hemodialysis
How is hemodialysis done?
How does the dialyzer clean my blood?
What sort of things are removed during dialysis?
How does my blood get into and out of my body?
What does the hemodialysis machine do?
What can I do during dialysis?
Why does the dialysis machine alarm?
What can happen during dialysis?
What are my jobs during dialysis?
What happens at the end of a dialysis session?
How long do hemodialysis treatments last?
Vascular access
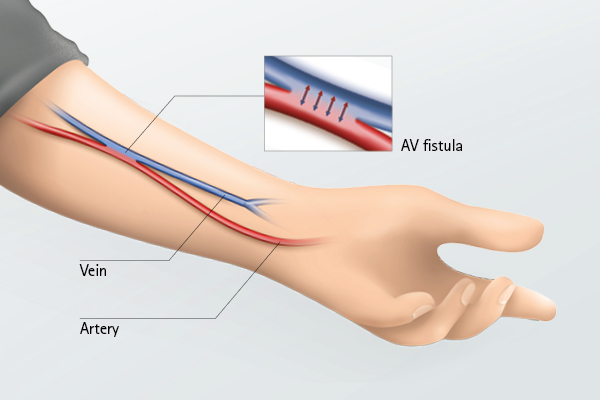
For dialysis to work properly it needs to create a way to take blood from your body, pass it through the dialyzer, where it is cleaned and then returned safely. Before starting your first HD treatment, an access to your bloodstream has to be prepared. This vascular access allows your blood to be easily taken from a vein in order to flow through the bloodlines to the dialyzer and back through bloodlines into the body. Therefore, such an access has to be surgically created in the arm, leg or near the collarbone. There are three main types of vascular access for hemodialysis treatment: The AV fistula, the vascular access graft as well as the central venous catheter.
Watch carefully for signs of infection: redness, swelling, pain, high pulse rate and fever. If you notice any of these signs, contact your renal care center immediately.
