Time to wake up!
The extent of the problem is enormous and alarming. The threat is real, it‘s here to stay, and the time to act is now.
Get an overview of the whole extent of the antibiotics crisis: how resistance develops, how it spreads and what role we all play - and what it all very specifically means today and in the future. Listen to and watch what leading experts have to say and the alternatives and smart solutions on which researchers are currently working to outwit highly adaptable pathogens. Scientists, governments and global organizations are collecting data, attempting to formulate rules and action plans, and implement programs to curb antibiotic resistance and its consequences.
The fight has already begun, its outcome has yet to be determined. To prevent falling back to the medical Middle Ages where every infection would potentially be a death sentence, every one of us needs to be aware of our responsibility - and face up to it.
Time to wake up. This is your wake-up call!
The problem of antibiotic resistance
What does “antibiotic resistance” mean to you? A severely ill patient in hospital, suffering from a germ that cannot be killed by any antibiotic known to man? This image is of course true, but it is only part of the picture. In reality, antibiotic resistance – or antimicrobial resistance, which as a broader term encompasses resistance caused by other microbes such as parasites, viruses and fungal diseases – does damage that goes far beyond the confines of the hospital. It is a truly global social problem that will affect us all sooner or later if we don’t act together to stop it. So let’s talk about it.
„This is a serious issue that is with us now, causing deaths. If it was anything else, people would be up in arms about it. […] We really are facing – if we don’t take action now – a dreadful post-antibiotic apocalypse.“
What is it?
Antibiotics are medicines used to prevent and treat bacterial infections. (They do NOT target viruses and are therefore utterly useless for viral infections such as the common cold.) Antibiotics target, attack and kill most of the bacteria involved.
However, some bacteria mutate and become resistant to those antibiotics. Consequently, they survive the antibiotic onslaught and spread the very mutation that makes them immune. And when these resistant bacteria infect humans and animals, they are much harder to treat than those caused by non-resistant bacteria.
In a lot of cases, doctors have run out of options altogether: In the European Union for instance, experts estimated that approximately 33,000 people die each year as a direct consequence of a bacterial infection resistant to antibiotics (https://ecdc.europa.eu/en/news-events/33000-people-die-every-year-due-infections-antibiotic-resistant-bacteria).
„Simply put, if we don’t address this problem now, we will no longer be able to treat common infections in the future. […] Some types of bacteria that cause serious infections in humans have already developed resistance to most or all of the available treatments.“
In a hospital environment, pathogens that develop antibiotic resistance are sometimes referred to as “superbugs”. (Probably because it takes the doctors’ superhuman effort to get rid of them.) Two main causes for antibiotic resistance have been identified: misuse (for instance against viral infections in humans) and overuse (for instance in agriculture).






How does it happen?
Bacteria can become resistant to antibiotics in several ways. Some bacteria can “neutralize” an antibiotic by changing it in a way that makes it harmless, and some have learned how to pump an antibiotic back outside of the pathogen before it can do any harm. Others can change their outer structure so the antibiotic has no way to even attach to the bacteria, let alone kill it.
If even one bacterium becomes resistant to antibiotics, it can then multiply and replace all the bacteria that were previously killed off. Exposure to antibiotics thus provides the so-called “selective pressure”, which makes the surviving bacteria more likely to be resistant. And the misuse and overuse of antibiotics – for instance when prescribed for a viral common cold – accelerates this process.
How does it spread?
The spreading of antibiotic resistance is an vicious cycle involving humans and animals. Poor hygiene, overuse and misuse of antibiotics all play a part.
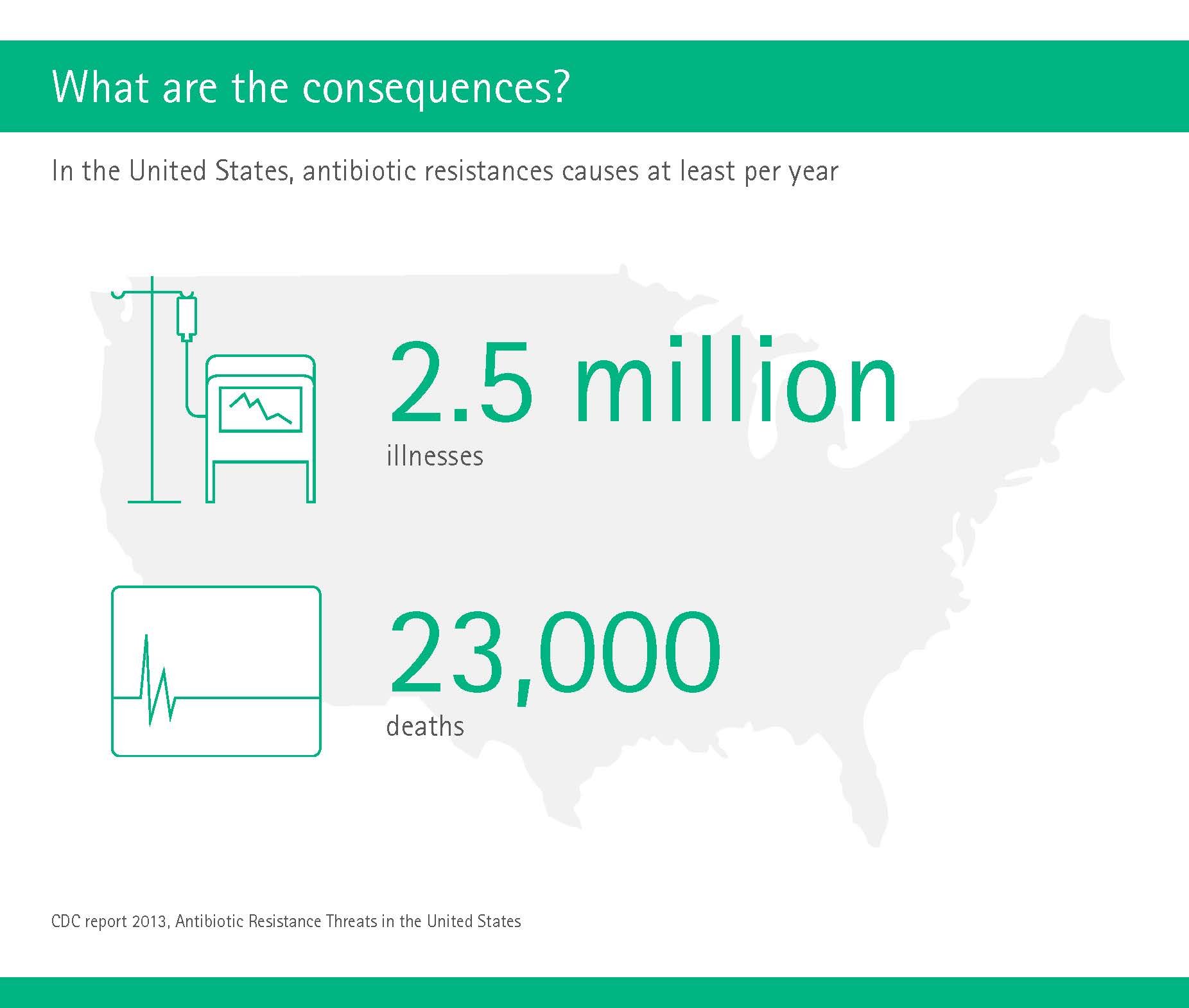
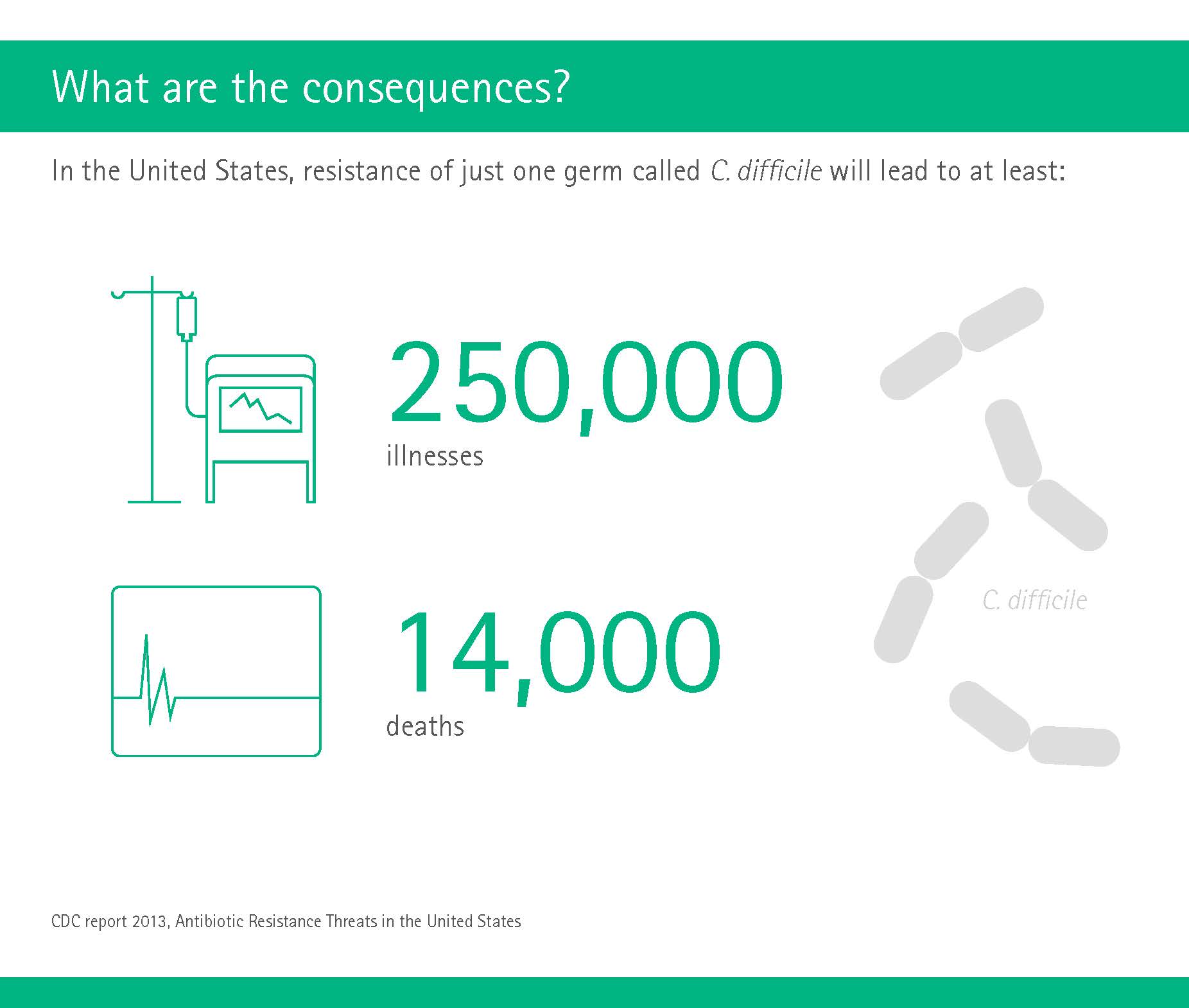
What are the consequences?
The issue of antibiotic resistance has been troubling experts more or less since they were first discovered. But in recent years, the numbers that researchers from all over the globe have compiled make for grim reading, and should provide the impetus needed to instigate meaningful changes worldwide.


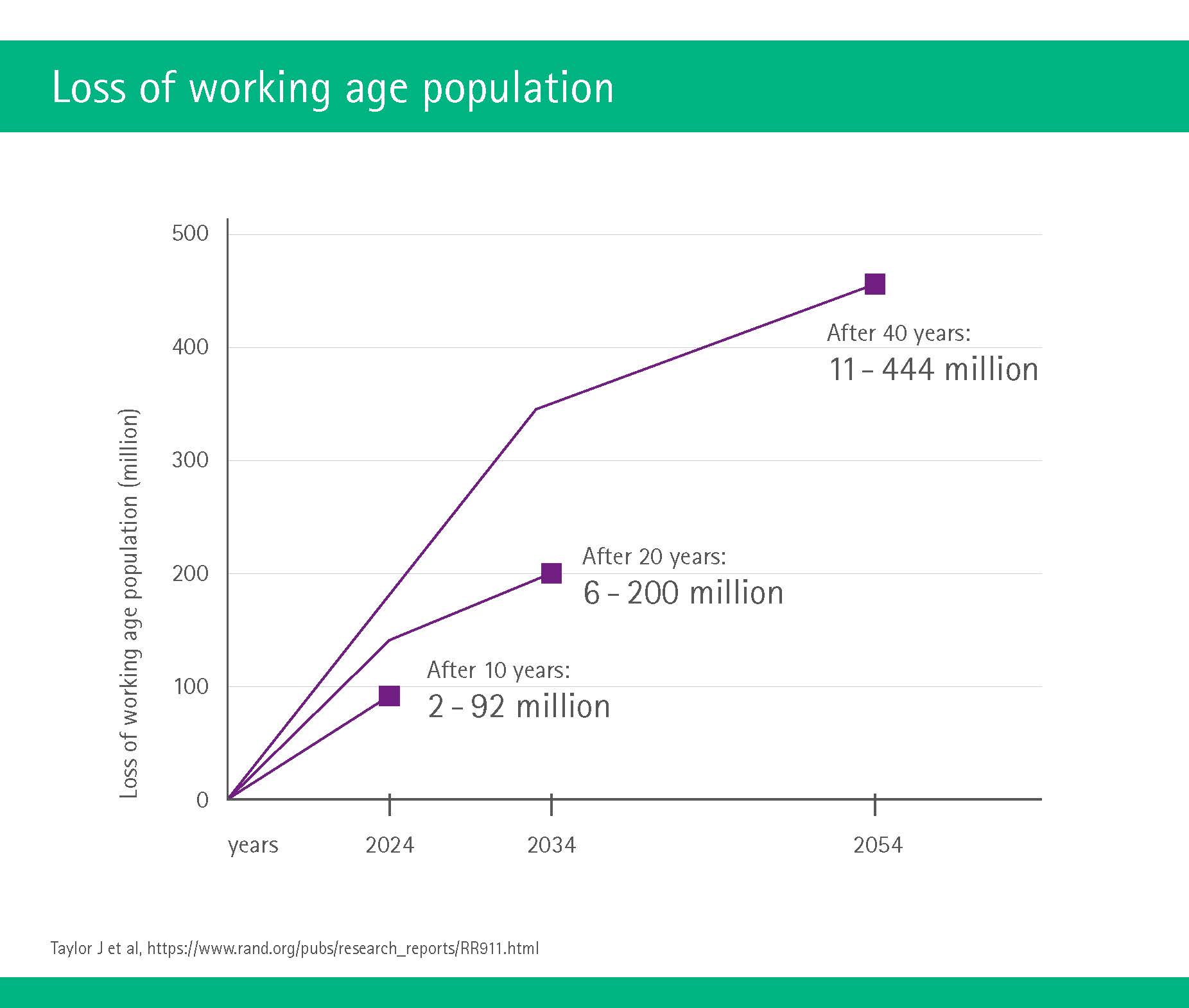
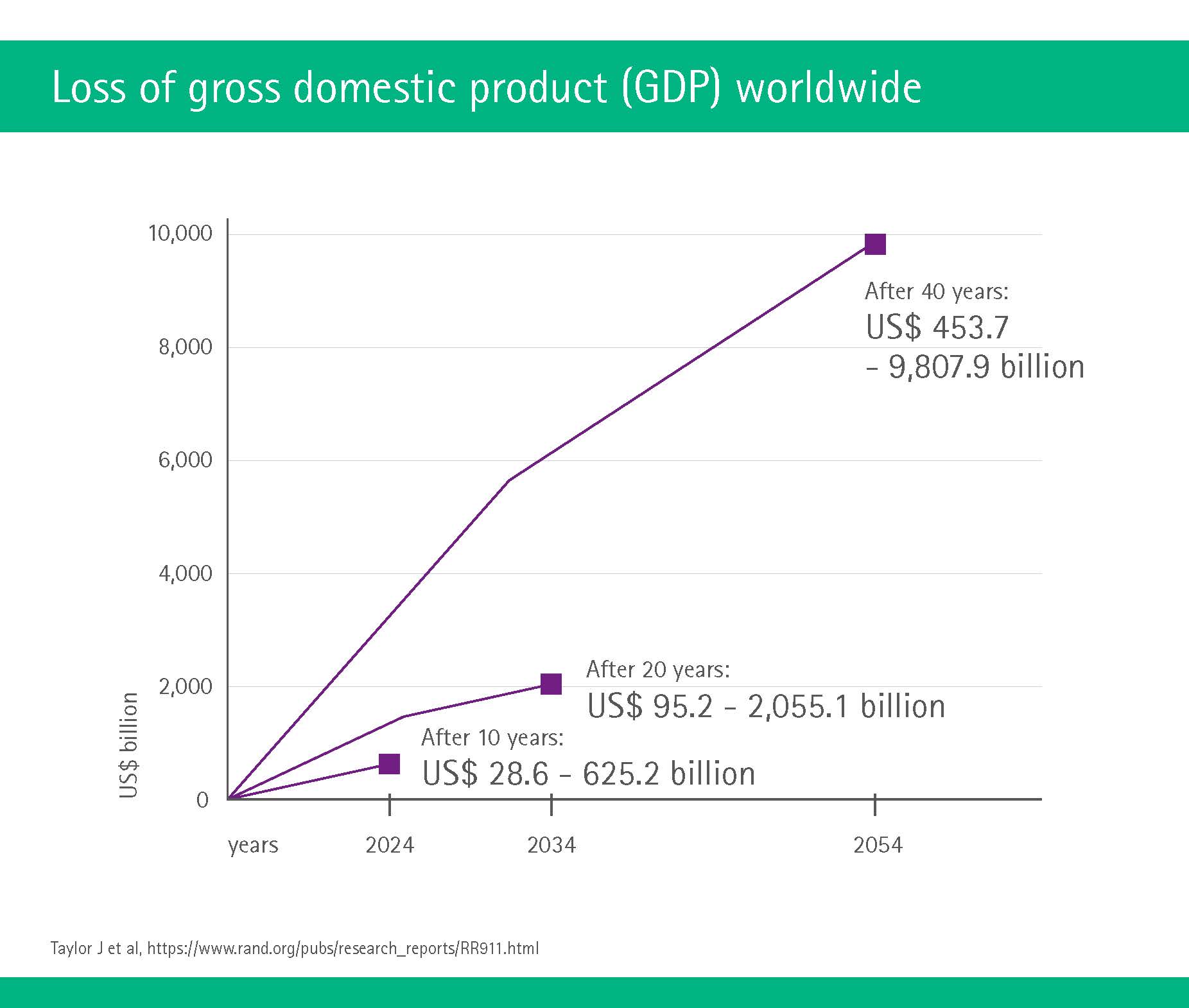
These are the data of today. In addition, researchers have estimated how antibiotic resistance and its consequences of disease and deaths would influence the world’s working population. They found that, compared to a world without antibiotic resistance, the world’s working age population would decrease drastically and the loss of gross domestic product would be significant.
„The scale and nature of this economic threat could wipe out hard-fought development gains and take us away from our goals of ending extreme poverty and boosting shared prosperity.“
So is it all doom and gloom? No, not least because there are measures that every person can take to help the situation.







Why is it so hard to develop new drugs?
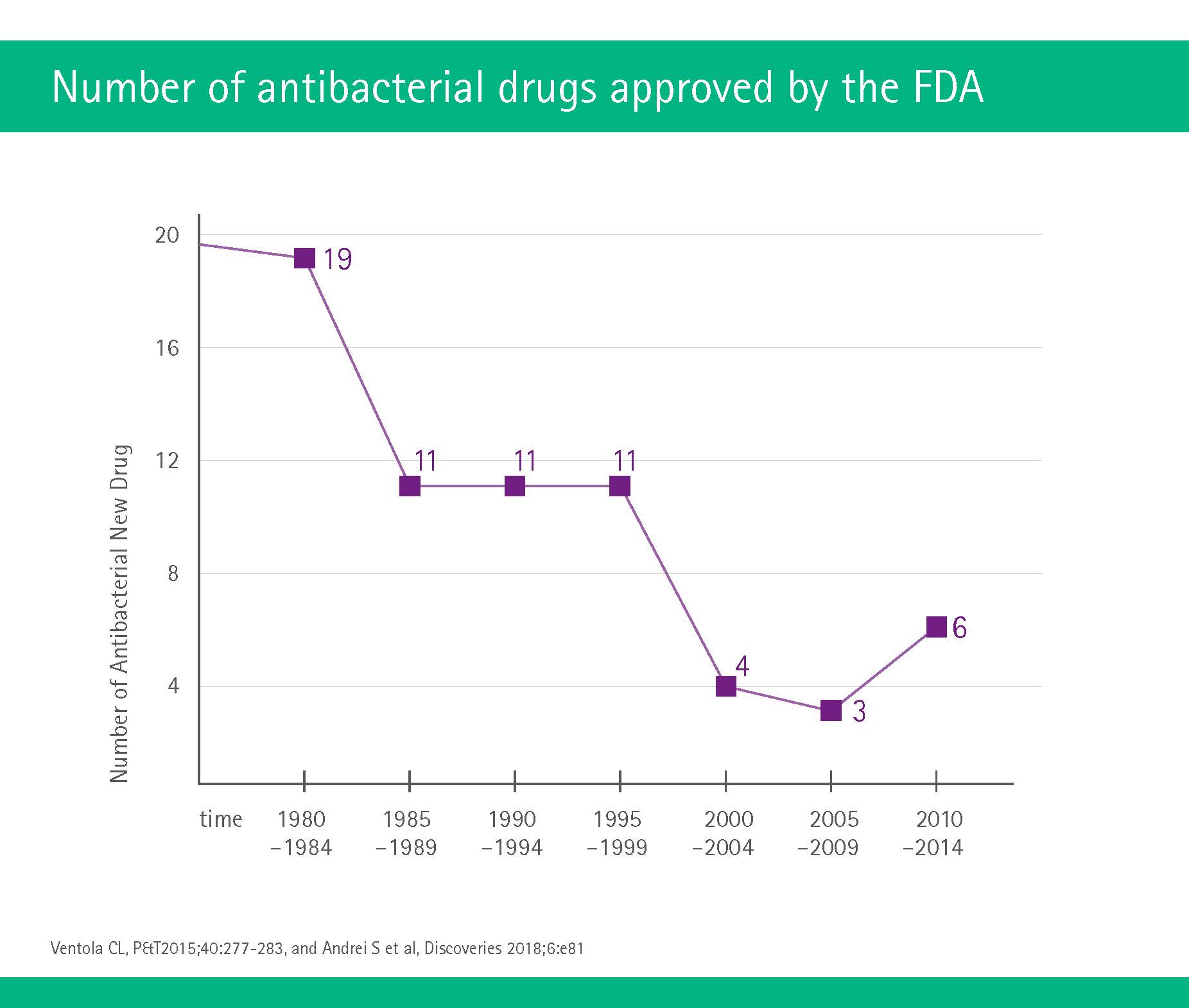
From the 1960s to the 1980s, pharmaceutical companies tried to counteract the issue by developing many new antibiotics. However, in the last few years, fewer and fewer antibiotics have been developed, steadily reducing the number of alternatives that can be used to treat germs that continuously develop new resistances. The pharmaceutical industry – both companies as well as institutes – are therefore called upon to renew their efforts to develop new antibiotics.
The good news is that some pharmaceutical companies have done just that. Also, researchers are more than ever exploring alternatives to antibiotics as well as boosters to increase the antibiotics’ efficacy, and governments worldwide have joined in the battle against the global antibiotic resistance. The next chapter will tell you more.
Medical solutions to antibiotic resistance
The issue should be simple. Surely, if one antibiotic no longer works, it should be easy enough to develop a new one? Unfortunately, the situation regarding antibiotics is a bit more complicated. A quick dip into history will show why, and a slightly longer dip into the future will show how scientists are dealing with the issue.
„We are already seeing infections that are resistant to all antibiotics – this is well known. Therefore, we must work extremely hard to safeguard the medications that are critical to human health, and facilitate research and development of new drugs.“



You could call it an ancient ping-pong match between bacteria and science: Whenever scientists have developed or invented a new drug, bacteria have responded with adaptions that allow them to become resistant – until the next compound comes along. These adaptions can take a variety of forms.
New antibiotics: Setbacks and successes
In recent years, scientists have increased their focus on trying to develop new antibiotics; some of which have had more success than others. For example, in 2015 researchers hailed the discovery of two new antibiotics: Gulmirecin and disciformycin A and B were thought to be very effective against some bacteria already resistant against certain antibiotics. Unfortunately, the enthusiasm seems to have been unfounded, as no new studies have since been published on this subject.
However, another antibiotic, also discovered in 2015 and called teixobactin, has just been used successfully to treat infections in mice (animal studies are always the first step before testing drugs in humans). The researchers hope that teixobactin will be available as a drug in six to ten years’ time (https://newatlas.com/new-novel-antibiotic-success-animal-testing/53943/).
And yet another antibiotic drug, the aptly named malacidin (“mal” = bad, “cide” = to kill), was recently observed to break down the cell walls of the still-dreaded MRSA pathogen mentioned above (Hover BM et al, Nature Microbiol 2018;3:415-422). The team behind this discovery is now working to make malacidin available for mass production – which could take a while.
Breaking the resistance
In addition to new antibiotics, scientists have also looked at other options. For instance, non-antibiotic ‘adjuvant’ compounds, also known as ‘resistance breakers’ or ‘antibiotic potentiators’, can be administered together with the antibiotic. They act to block the resistance or to enhance the strength of the antibiotic. These drugs may be new entities or a compound that already exists. Three main types of antibiotic adjuvants have been developed so far, and their names accurately reflect their methods of action (Gonzáles-Bello C, Bioorg Med Chem Lett 2017;27:4221-4228: Beta-lactamase inhibitors, efflux pump inhibitors and outer membrane permeabilizers.)
Bacteria-eating viruses
Another option is the so-called phage therapy using ‘bacteriophages’ – basically viruses that eat bacteria. For 100 years, they have proven themselves in the treatment of wounds or infections, but with the growing dominance of static drugs such as antibiotics, phage therapy fell into disuse. Their manufacture is elaborate and difficult and it is complicated for phages to be patented: Because just as bacteria are changing, it is also necessary for the viruses that combat them to change, so a company would have to re-apply with every new phage-therapy.
This could, however, change with the antibiotic crisis: Eastern European researchers, where phages are most intensively studied and still in use, have started to work together closely with American scientists, and the National Institute for Infections in the USA has put phage therapy on the list of the most promising treatment strategies against bacteria.
Recently, researchers from University College London took the idea of harnessing viruses to use against bacterial infections one step further. They engineered an artificial virus that kills bacteria on contact – and unlike antibiotics, which target a single structure within the bacterial cell, the artificial version attacks the bacterium as a whole and destroys it within minutes (De Santis E et al, Nature Communications 2017;8:2263). This mode of action also means that bacteria are less likely to become resistant.
Plasma from the stars
Plasma is a state of matter, like a solid or gas. It is normally found in high-energy environments such as stars, but can also be artificially generated at lower temperatures by applying electrical currents to a gas or liquid insulator. The point is: Plasma can kill bacteria – including those that are resistant to antibiotics. Normally, plasmas form at high temperatures, but German scientists have managed to develop a patch that can create cold plasmas (https://motherboard.vice.com/en_us/article/qvnww3/these-plasma-patches-could-replace-antibiotics-to-treat-chronic-wounds).
These ‘cold plasma patches’ are made of silicone, and use the ions and UV radiation emitted by the material to treat infections in chronic wounds, while simultaneously accelerating the healing process. Basically, it is ionized, bioactive gas that can kill bacteria within minutes. The downside is: These patches can only be used for external infections such as skin wounds. In these cases, they may replace the need for antibiotics.
Orchids, sloths and crocodiles: What’s next?
Scientists are increasingly looking for solutions to the antibiotic resistance problem in unusual places – or at least places you would not immediately associate with antibiotic resistance. These fascinating potential sources of new antibiotic drugs cover a wide range from orchids to sloth hair to leafcutter ants to Komodo dragons. None of these discoveries have yet made it to the final stage of delivering a new drug, but first insights look promising.







It seems evident that not all of these investigations will lead to the development of new drugs in the fight against antimicrobial resistance, but without trying, we shall never find out. And at the very least we could spare a thought for those brave scientists politely asking crocodiles for a blood sample or trying to get cuddly Komodo dragons to lick a cotton swab without having their hand bitten off.
Smart solutions in the fight against infections
As the ultimate security provided by antibiotic resources has come to seem ever more dubious, new innovations are being leveraged in order to cope with the age-old imperative of killing germs that attack humans. These include so-called real-time locating systems, the use of (UV-) light for disinfection and virtual reality technologies.
Smart systems are watching
Real-time locating systems, or RTLS, are known as “GPS for indoors”. Why? Because they allow the user to both identify and track different items through a given environment. This has multiple advantages, from the mundane – having to spend less time looking for things – to the life-saving, for instance when hospitals need to quickly identify personnel who have come into contact with a contaminated patient.
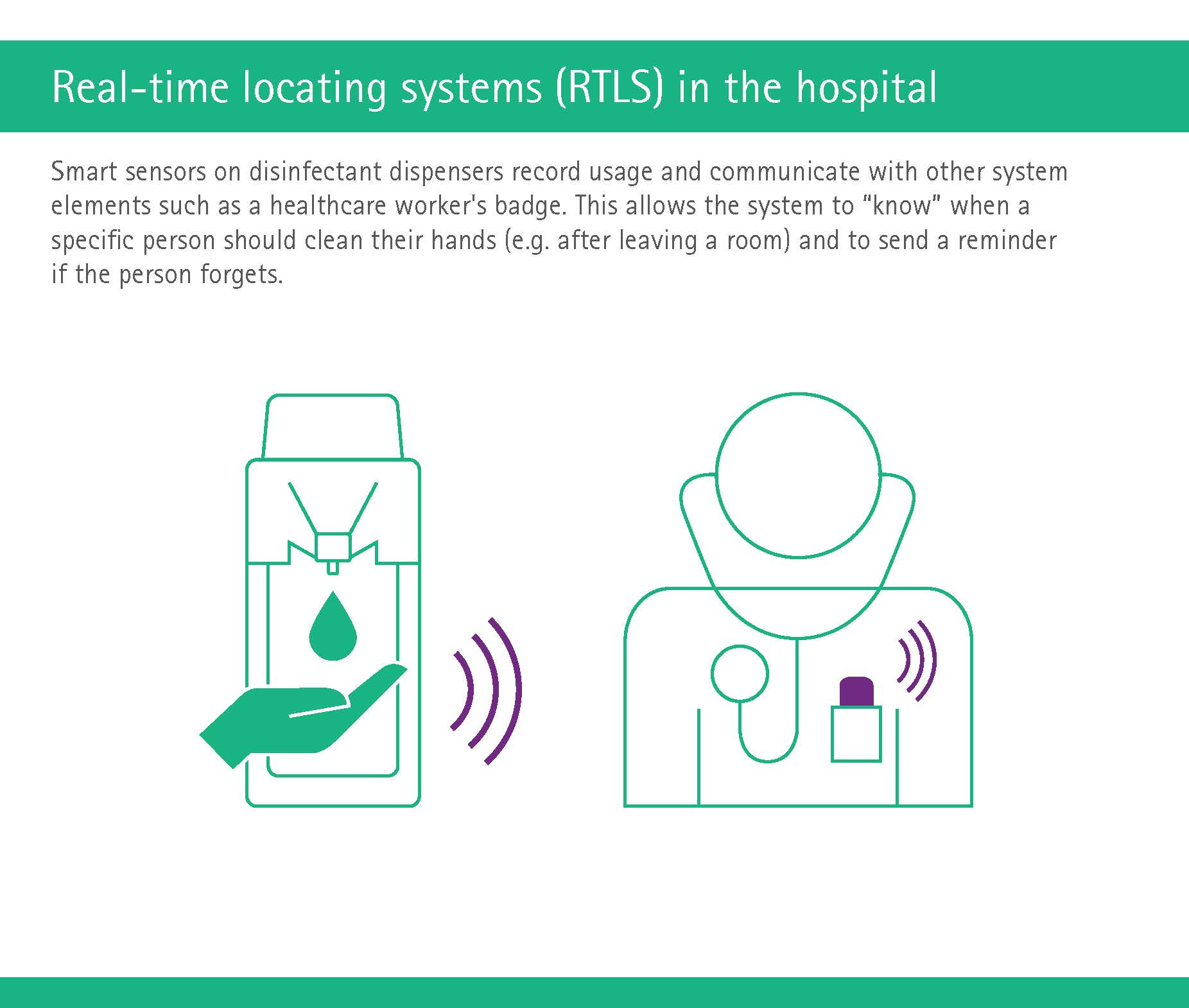
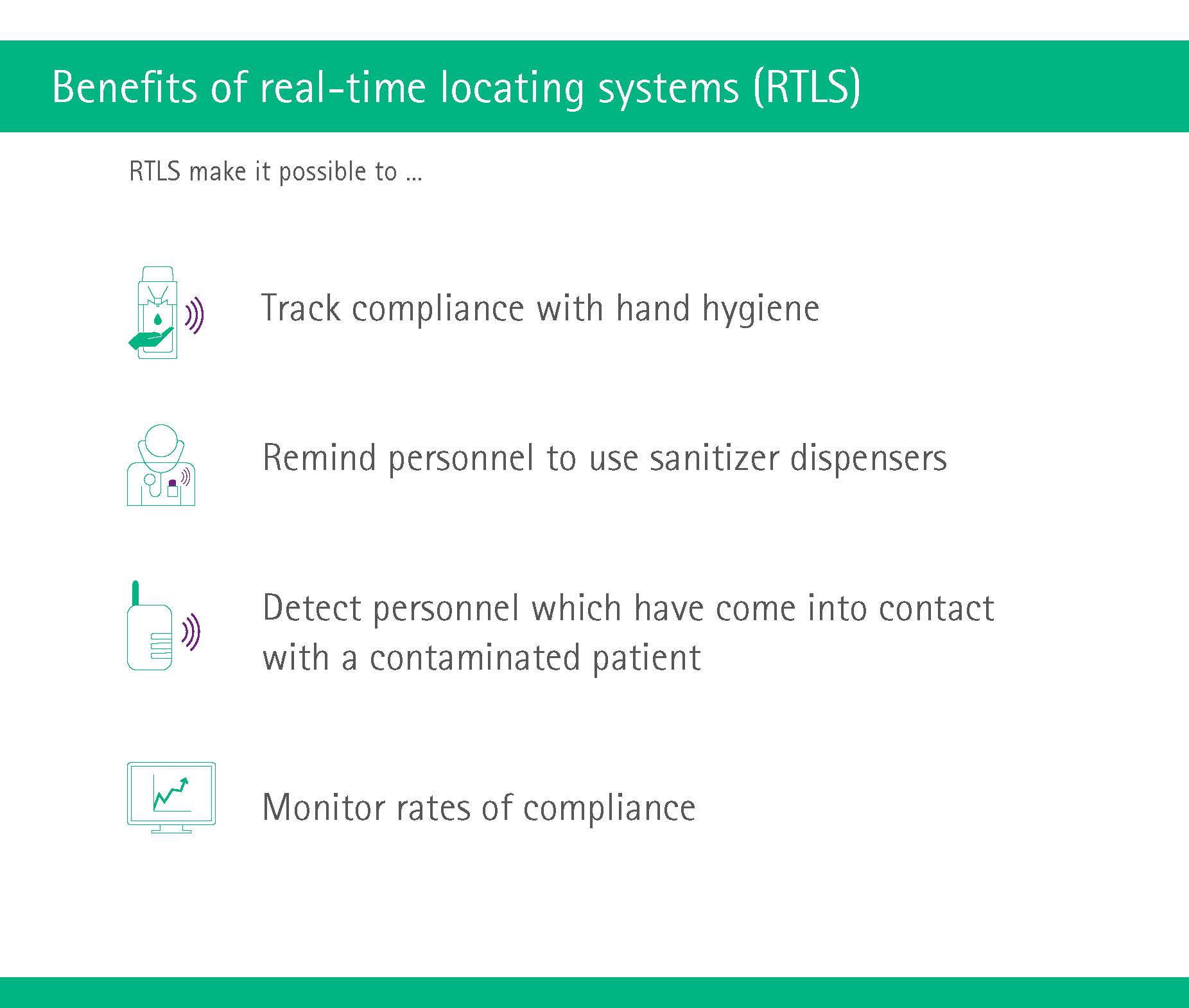
Smart systems also come in handy with respect to hand hygiene, or more specifically, compliance to hand hygiene, which in most countries is still not where it should be. For instance, some hospitals install sensors on disinfectant dispensers that record usage and communicate with other system elements such as a worker’s badge. This allows the system to “know” when a specific person should clean their hands (e.g. after leaving a room). If the person forgets, a short alarm will sound. (And if you think these monitoring systems are slightly creepy, just search online for images of MRSA infections – they are way more horrible.)
Germicidal lamps
The germicidal effect of ultraviolet (UV) light was first discovered in the latter part of the nineteenth century; by the 1950s, it was being used to disinfect drinking water in water treatment systems. Now, the disinfecting properties of UV and other light have sparked new interest as a way of improving hospitals hygiene.
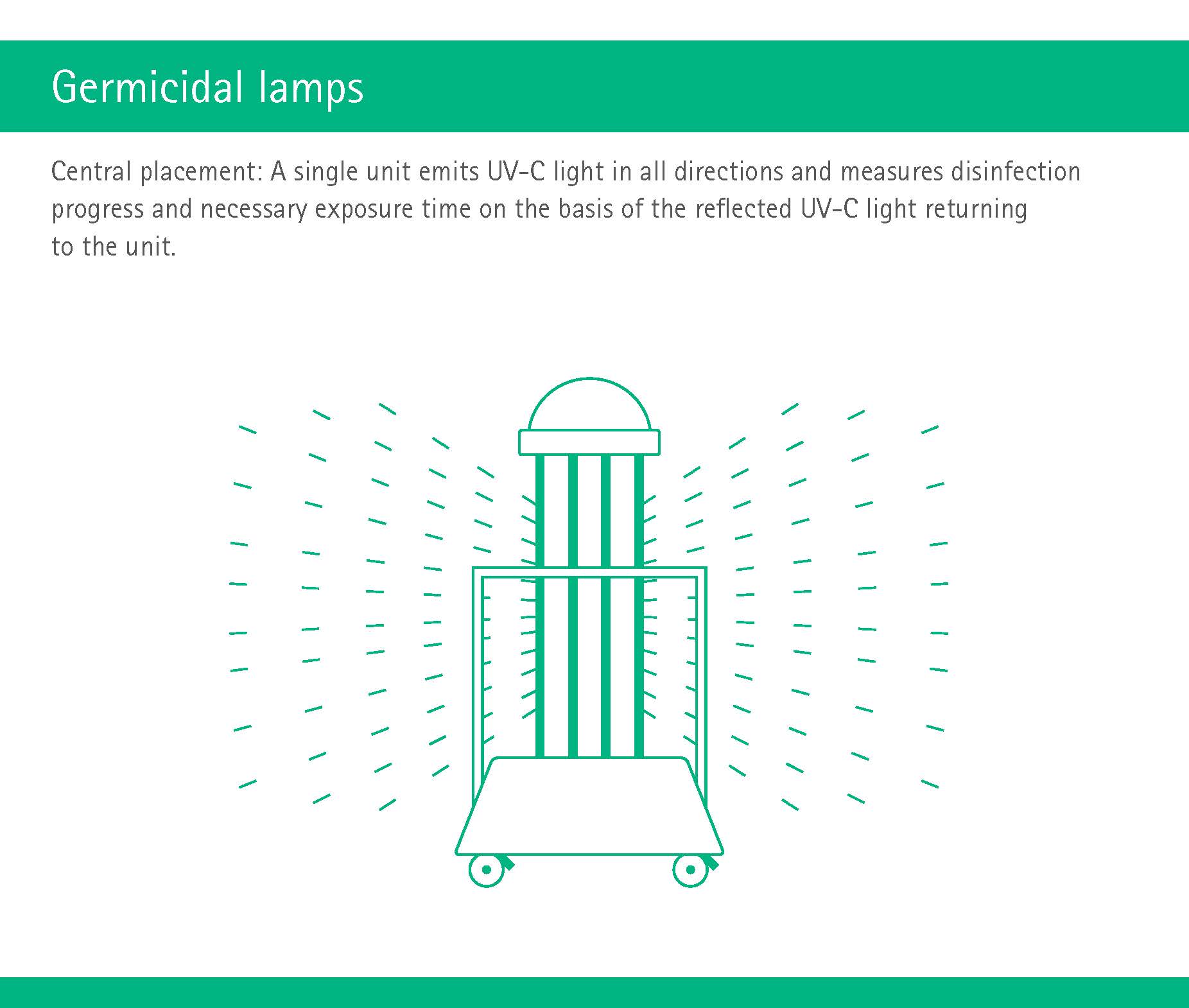
For instance, robots that emit high-intensity UV light in short time periods are used to disinfect whole rooms in hospitals. The UV light kills various pathogens (including the potentially lethal MRSA) by altering their DNA and rendering them unable to reproduce. One hospital conducting a 3-month trial of this technology found a significant downward trend in hospital-acquired infections caused by the bacteria Clostridium difficile.
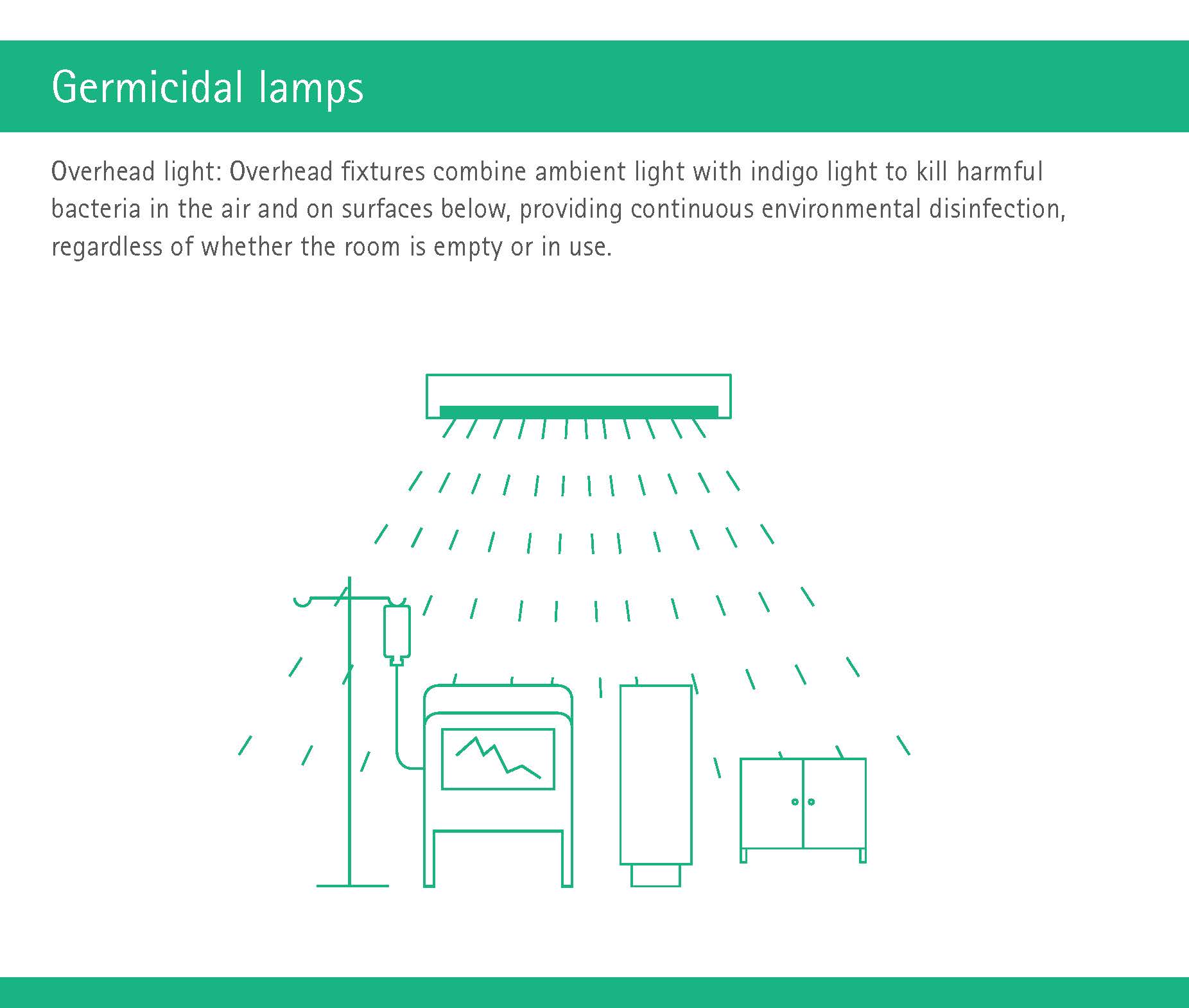
Other hospitals have implemented motion-activated overhead light fixtures in their operating rooms. These fixtures combine white ambient light with indigo light to kill harmful bacteria in the air and on hard and soft surfaces below. As a result, they provide continuous environmental disinfection, regardless of whether the room is empty or in use.
The advantages are clear: Classical whole-room disinfection systems require a member of staff to wheel a device into the OR and activate it; by contrast, overhead lights provide continuous environmental disinfection. With this approach, one hospital reported a 70 percent reduction of bacterial burden.
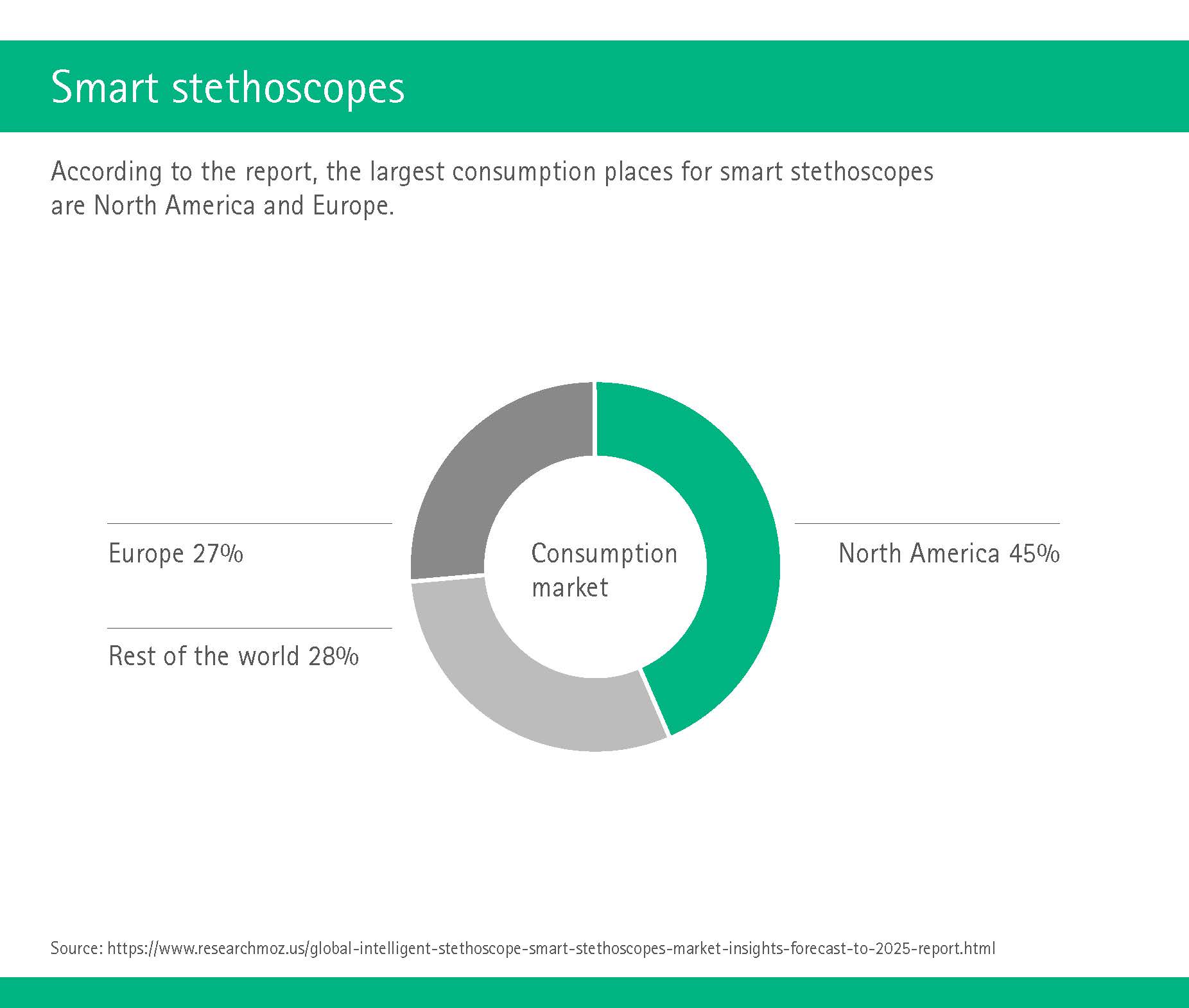
Smart stethoscopes
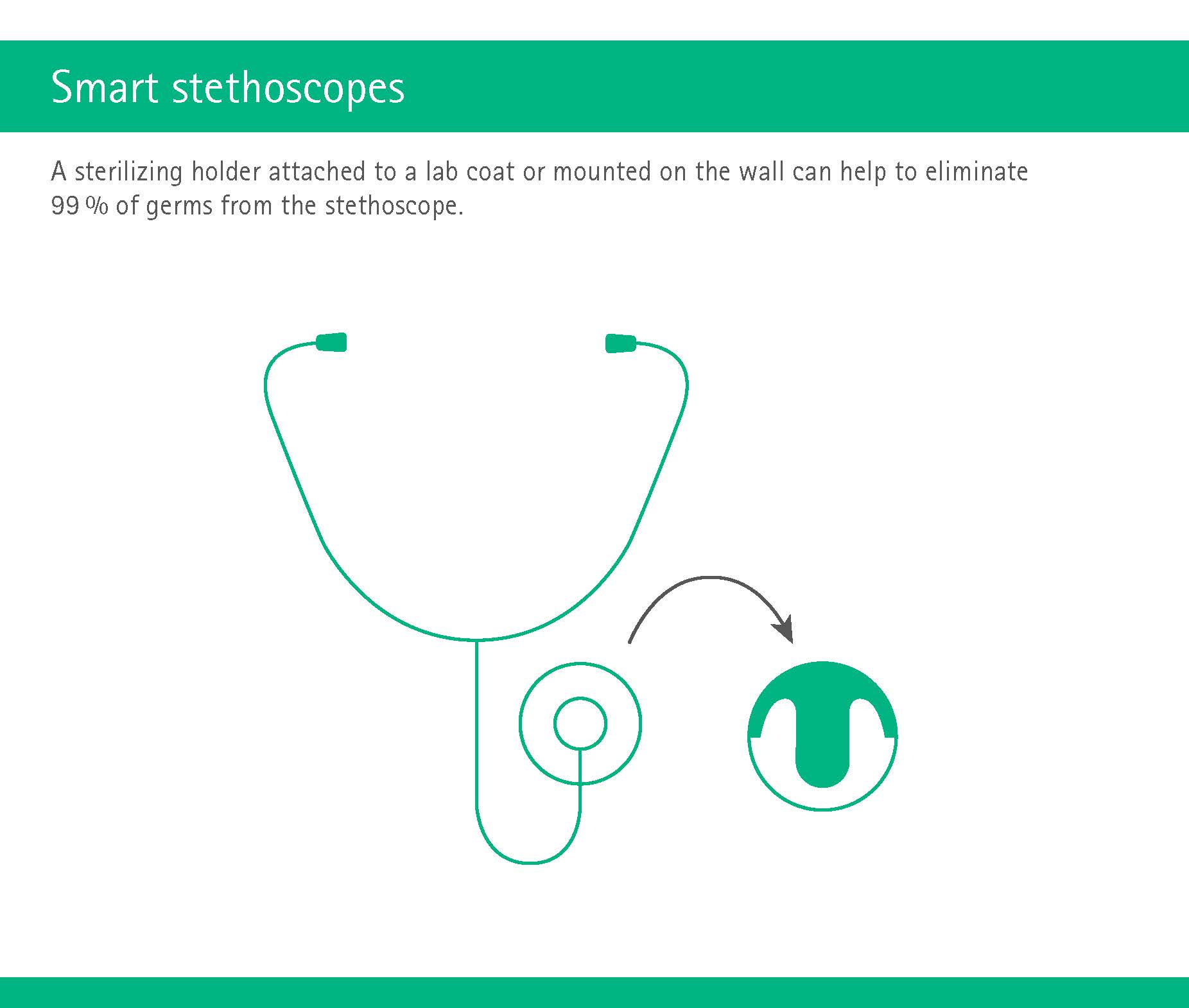
However, it does not always have to be shiny new things such as robots – smart things can be done with fairly old stuff too, such as stethoscopes. These key tools are as dirty as a physician’s hands, but cleaning them is often forgotten. Enter smart technologies such as a sterilizing magnetic holder that can be attached to the physician’s clothing. The stethoscope clicks into the holder, which contains an aseptic sponge; sliding the diaphragm across this sponge eliminates 99 percent of the germs. (http://cleanint.com/cleanstethoscope/).
Another possibility is a sterilizing device mounted on the wall: The physician swipes the chest-piece of the stethoscope with a “credit-card” type motion through the device, which then UV-sterilizes the stethoscope (http://www.uvs-ultraclean.com/stethoscope.htm)
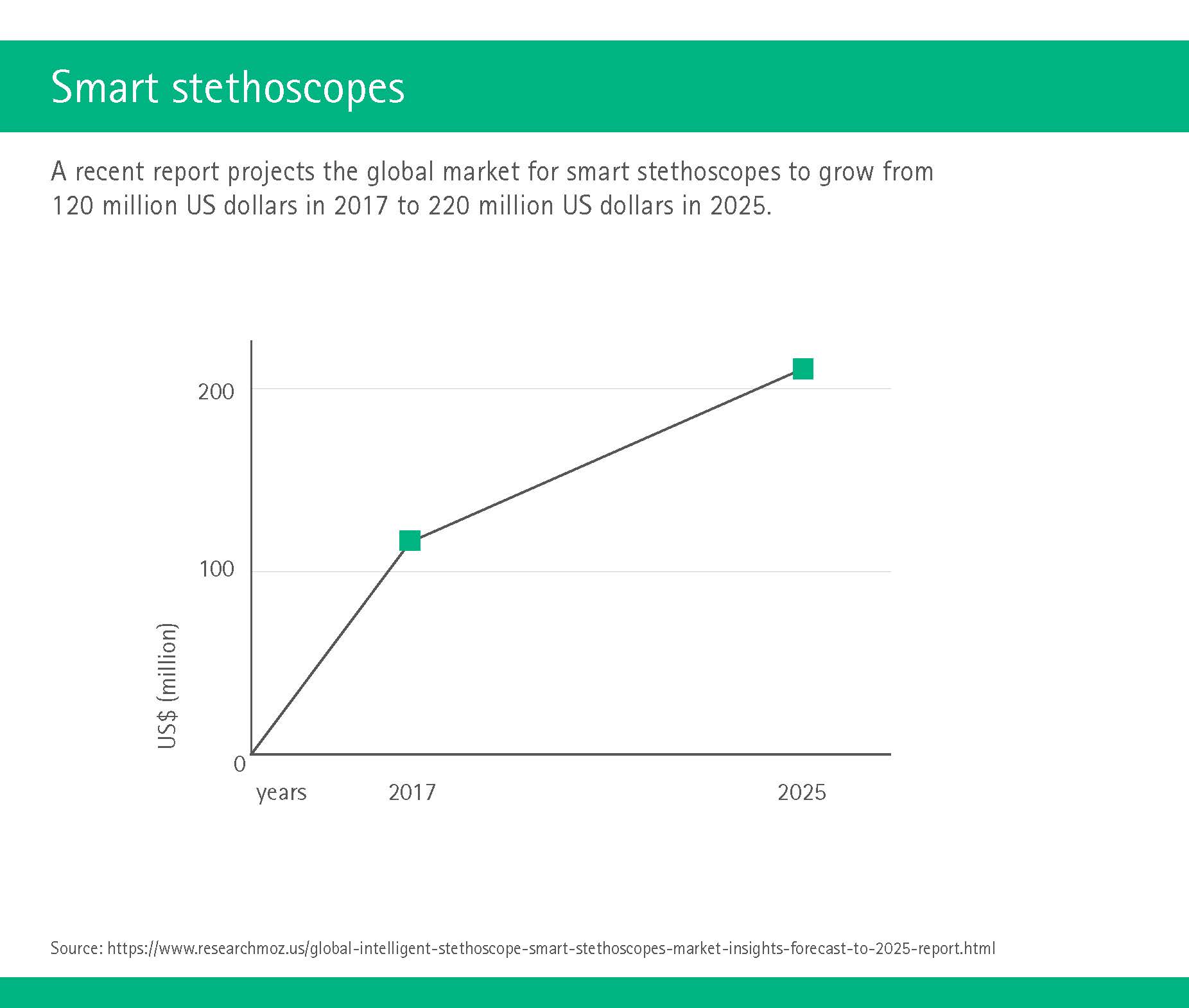
And these are not just niche products anymore: A new market study estimated that the smart stethoscopes market would reach US$ 220 million in 2025, with big-name companies at the forefront. (https://www.researchmoz.us/global-intelligent-stethoscope-smart-stethoscopes-market-insights-forecast-to-2025-report.html)
Systemic approach to room cleaning
Germs love to latch on to seemingly unimportant items such as door handles and toilet roll holders. Cleaning staff have the unenviable task of removing germs and other stuff from these fixtures, yet they are often overlooked in strategies of infection prevention. Systematic cleaning gives cleaning staff clear instructions on how to proceed. For instance, the instructions for cleaning the operating room might include “start top to bottom, clean from edge to center”, disinfect “every nook of every vent” and “validate the work with bioluminescence”.
Virtual reality for hospital design and hygiene
Virtual reality (VR) is probably not immediately associated with antibiotic resistance, yet it could play an important part in trying to alleviate this issue. Starting with the design of a hospital: Imagine if doctors, nurses and hygiene specialists could don a pair of goggles and take a virtual stroll through their workplace before it has even been built. This would allow all parties to give valuable feedback on how to optimize the proposed design – also with the aim of improving hygiene management.
On the subject of hand hygiene (compliance), a VR hand hygiene simulator allows training simulation in three phases: i) a tutorial phase to teach the WHO “5 moments of hand hygiene”, ii) an interactive training phase in which the trainee is asked to evaluate the hand hygiene of a virtual nurse, and iii) a feedback phase in which the trainee receives a score. (https://pdfs.semanticscholar.org/presentation/b5e9/aa72daa86a3081a7c527a73cee43b86191bc.pdf).
VR is also increasingly used to train medical students, for instance regarding infection prevention in the operating room. This training is usually difficult to organize – one OR only has room for so many students, and those in the back will end up not seeing much. But VR allows a virtually unlimited (pun intended!) number of students to immerse themselves in the OR environment, study risky situations and learn how to avoid them.
Systemic solutions to antibiotic resistance
After our foray into smart solutions, let’s now look into some systemic approaches to the problem of antibiotic resistance. Since germs laugh at the idea of borders before crossing them, initiatives need to be implemented on all levels: global, national and individual.
Because the true extent of the problem has only been known for some years, quite a few of the programs are still at the stage of gathering data or implementing first changes – which means that there is still a lack of hard data as to the success of some of these programs. Nevertheless, promising projects are on the rise: governments, scientists and industries have taken up the gauntlet and are prepared to do battle. The game, ladies and gentlemen, is on.
First step to any solution: Data collection
The world leader on global initiatives is, unsurprisingly, the World Health Organization WHO. Their “Global Action Plan” has five objectives: Improve awareness and understanding of resistance, strengthen the all-important evidence base, reduce the incidence of infections, develop the business case for sustainable investment, and optimize the use of antibiotics in humans and animals.
For the last aim, the WHO works together with the OIE, the World Organization for Animal Health, which recently reported a first success: The number of countries not using antibiotics for animal growth increased from 86 (58.9% of all countries surveyed) in 2016 to 110 (70.9% of all countries surveyed) in 2017. (https://cddep.org/blog/posts/weekly-digest-feb-22-2019/)
„Human, animal, and environment health are all equally responsible for the correct use of antimicrobials and to avert the threat of antimicrobial resistance. As we strive to ensure that these medicines are rightly used in the community and in healthcare settings, one sector alone will not solve the problem.“
The WHO was also the first to publish a global report on surveillance data, which trumpeted the alarm bells in 2014: Even back then, there were “high levels of resistance” found in all world regions, and “significant gaps” existed in tracking antibiotic resistance. (https://apps.who.int/iris/bitstream/handle/10665/112647/WHO_HSE_PED_AIP_2014.2_eng.pdf;
jsessionid=F028BC0135BD98C6673BB1220D684DBD?sequence=1)
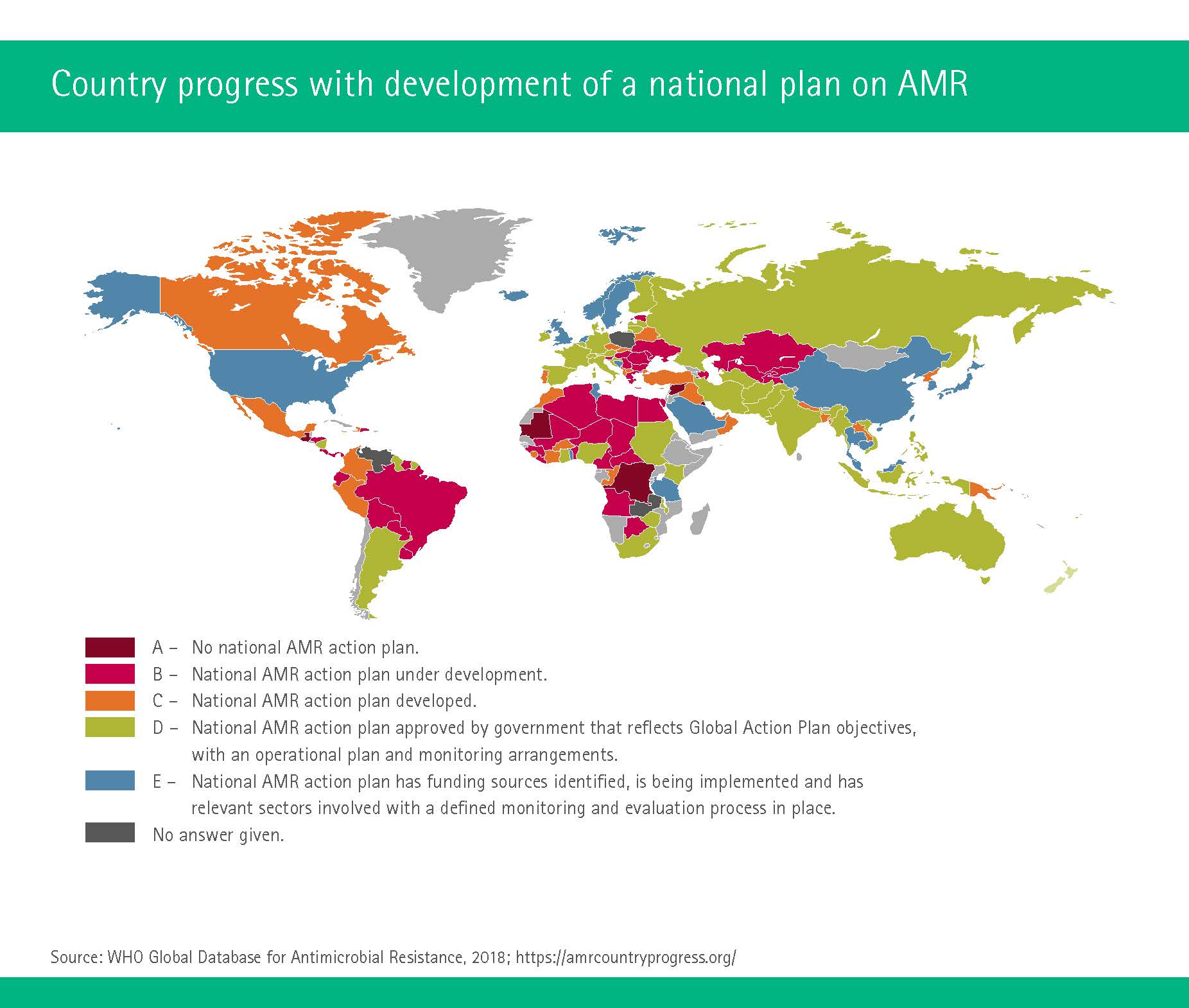
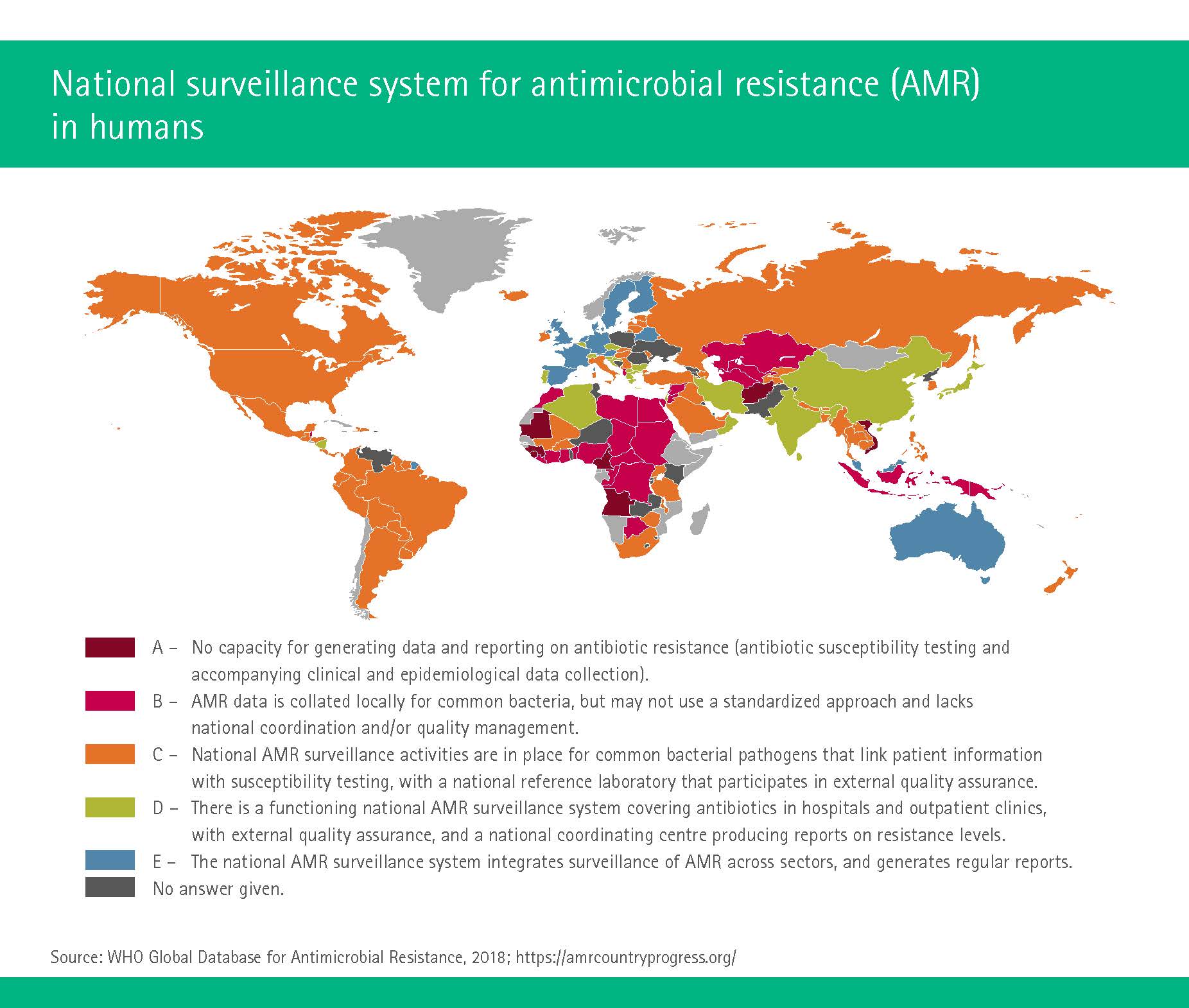
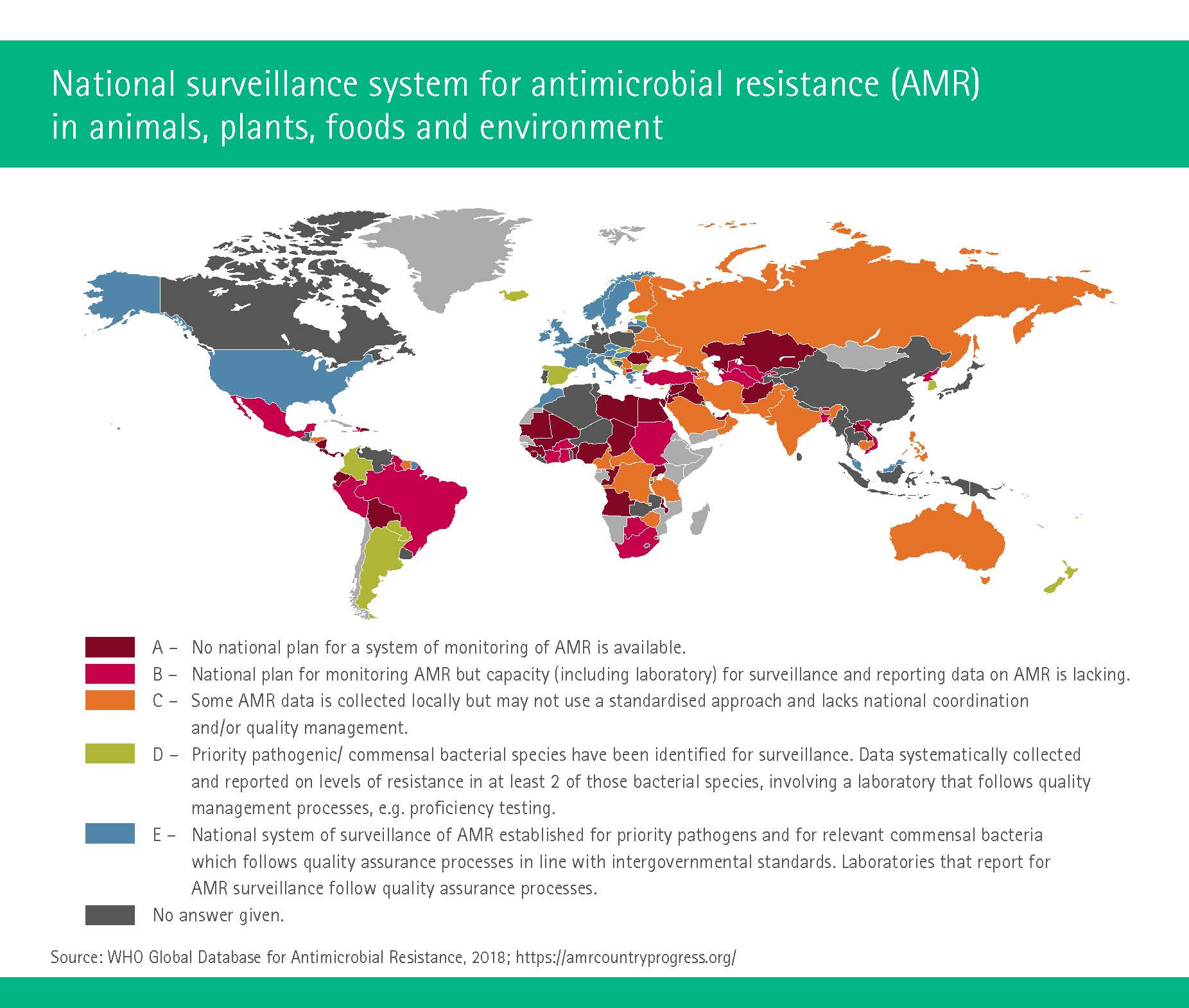
These data gaps at least are starting to narrow. In 2017, the WHO published a global database that allows an overview of where countries stand with respect to issues such as:
- Who has developed or implemented a “National Action Plan”: In Europe, only Austria, Switzerland, Italy, Portugal, Norway, Finland and Serbia have such a plan.
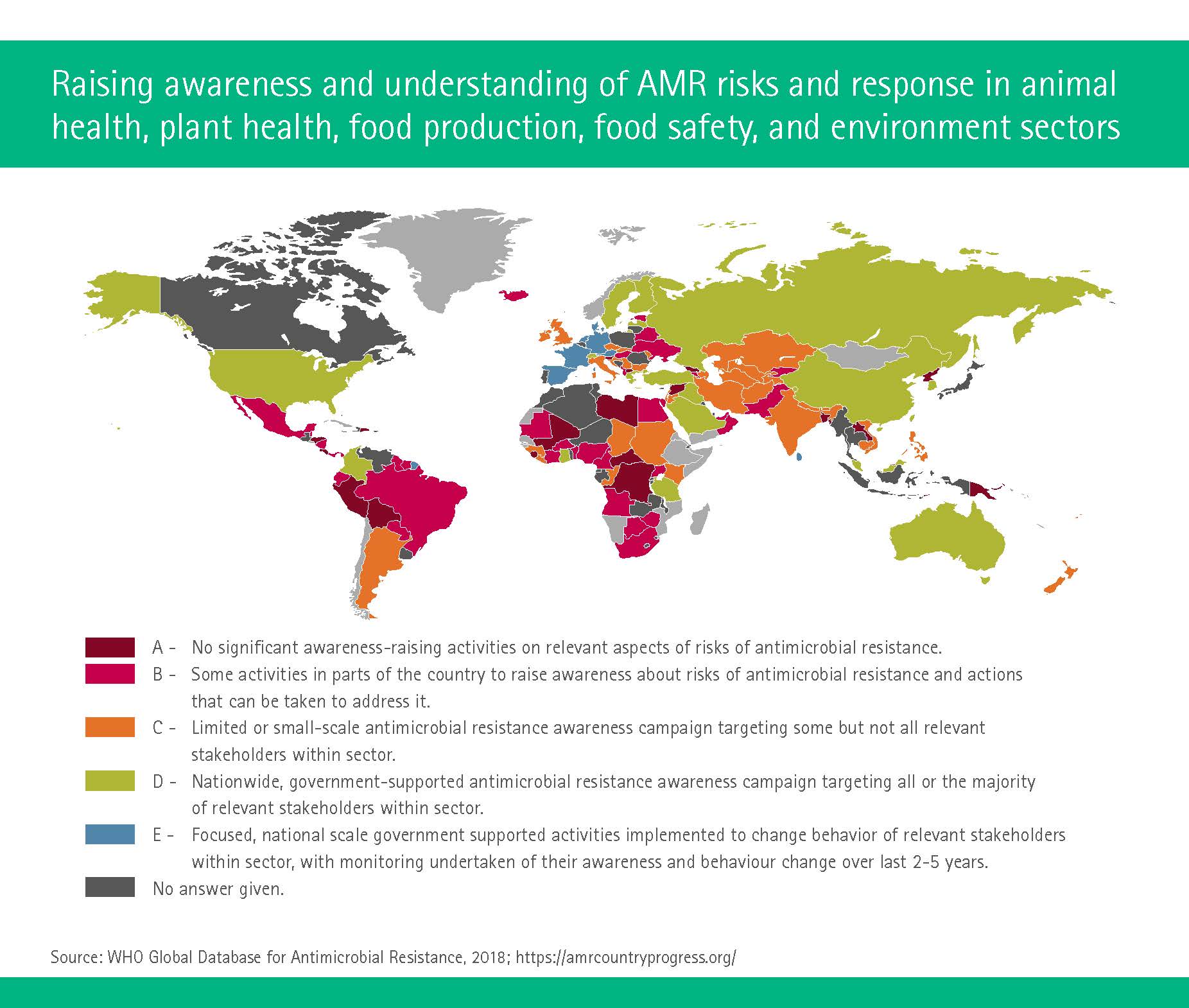
- Who trains professionals regarding antibiotic resistance in the veterinary sector: In Africa, only Botswana and the Ivory Coast have training courses available, and only South Africa, Kenya and Zimbabwe cover this issue in the curricula.
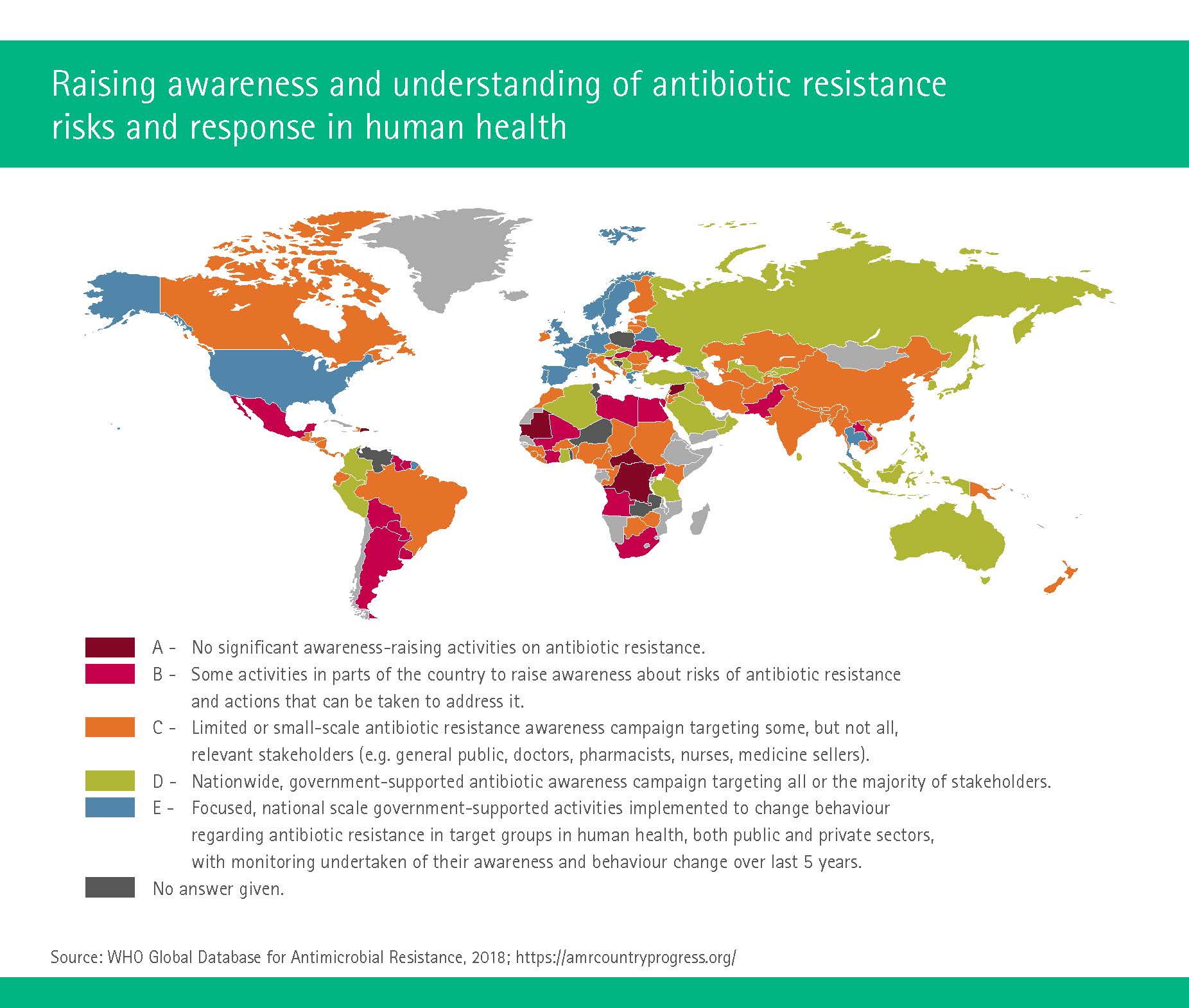
- Who is currently raising awareness and understanding of resistance risks in human health: The good news is the only countries on earth without such activities are Mauritania, Democratic Republic of Congo, Central African Republic and Syria) (https://amrcountryprogress.org/).
Unfortunately, the new data have also shown that the high levels of resistance are only going one way, and that is up. The first official “GLASS” (Global Antimicrobial Resistance Surveillance System) report was launched in 2015 and included 52 countries. Even then, the experts pointed to disturbingly high resistance levels across the 22 countries that were already reporting statistics. Widespread resistance was found in around 500,000 people, reports Dr. Marc Sprenger, Director of the WHO’s Antimicrobial Resistance Secretariat. “Of course, the situation is different from country to country, but there are several infections that are untreatable, meaning that patients can die from them – that is quite a dramatic situation.” (https://news.un.org/en/tags/global-antimicrobial-surveillance-system-glass)
The one good piece of news is that compared to the first data call in April 2017, in 2018 GLASS announced a 64 percent increase in country enrolment and more than twice the number of countries submitting antibiotic resistance data. Clearly, governments all over the globe are realizing that you have to join forces to beat antibiotic resistance. (https://www.who.int/gho/glass/en/)
„Since the rates of antimicrobial resistance, the rates of antimicrobial consumption as well as infection prevention and control practices vary from country to country, it is essential to tailor strategies to address specific needs.“
Room for improvement – everywhere
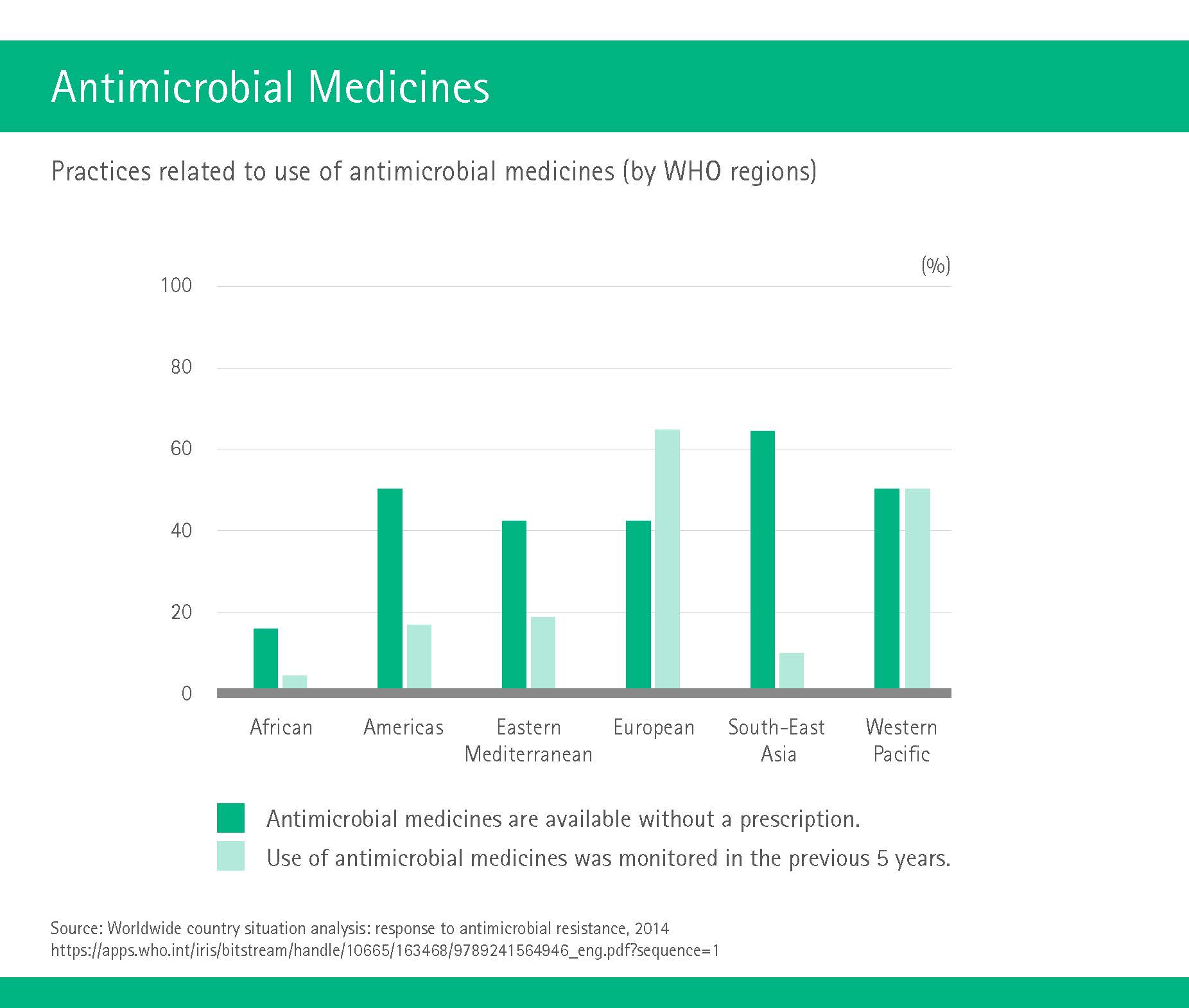
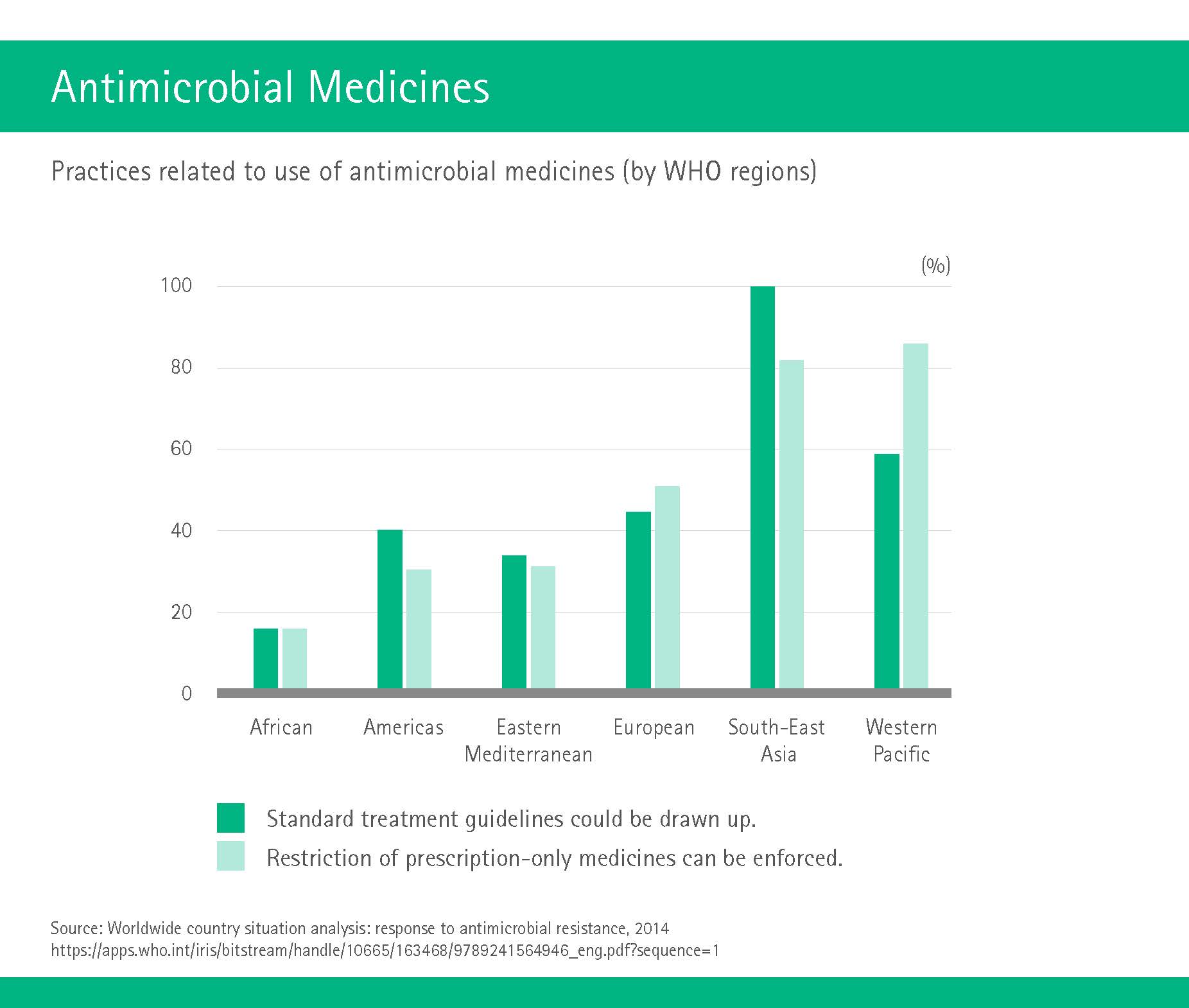
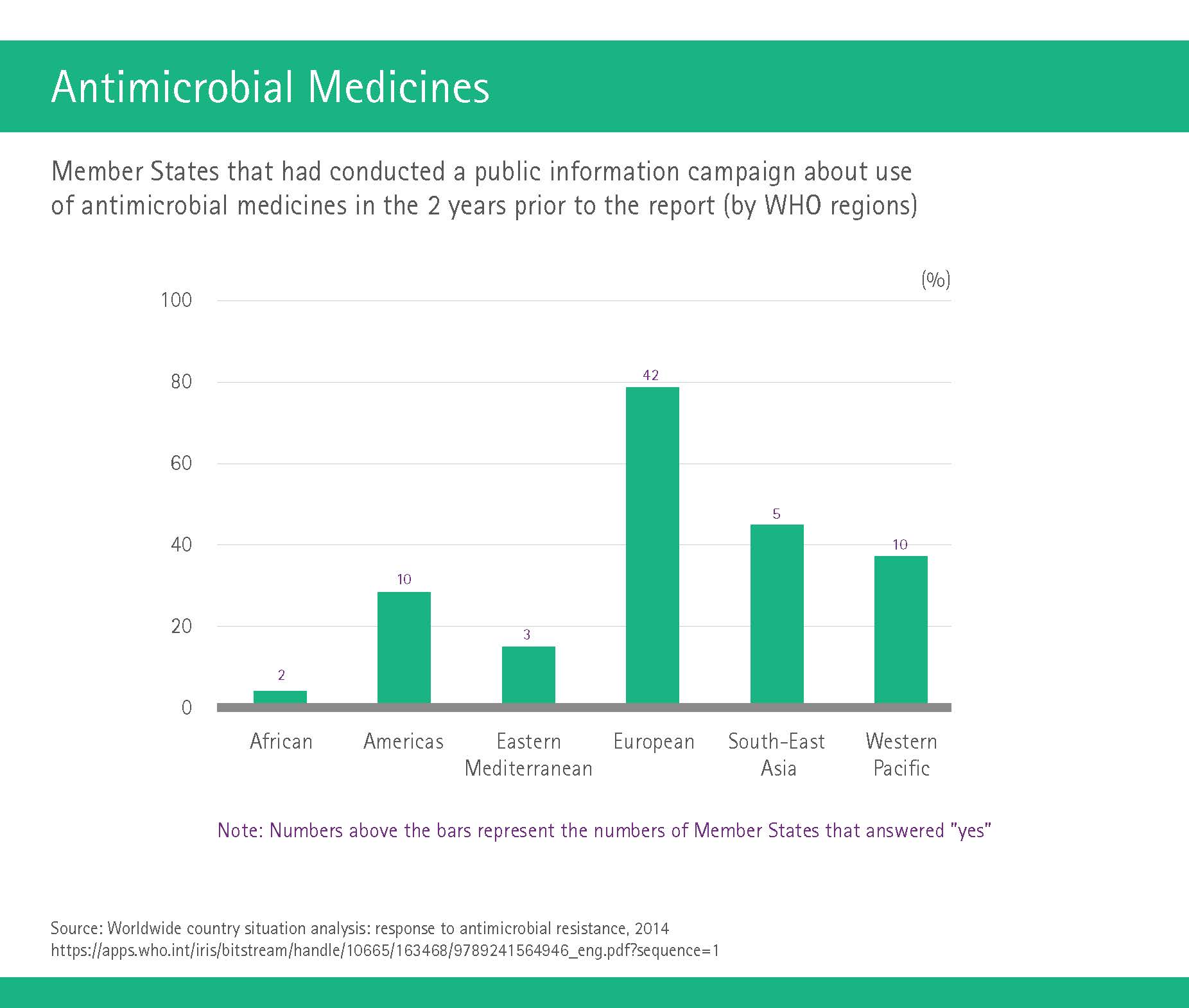
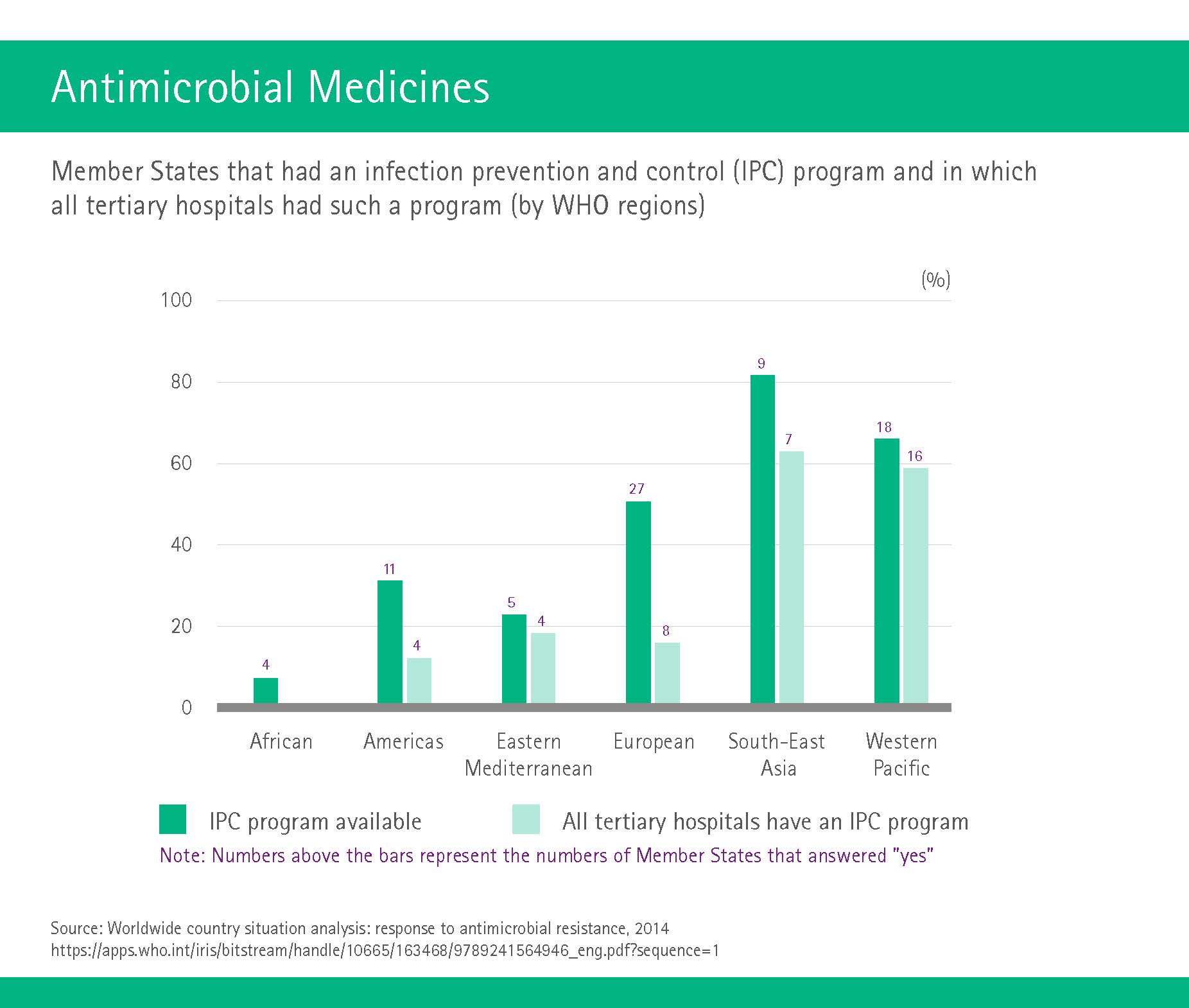
This should be all the more reason for countries to get their act together on a national level as well. As the WHO’s “Worldwide Country Situation Analysis” demonstrated, there is more than a bit of room for improvement here. Even in highly developed areas such as Europe, only 43 percent of countries have a national antimicrobial resistance plan. Antimicrobial medicines are available without a prescription in more than 50 percent of countries, including 51 percent of American countries and 64 percent of South-East Asian countries. African countries report a limited ability to enforce any existing regulations for use of these drugs in human medicine.
National plans for international bacteria
Some countries push ahead on their own: Canada has implemented a Federal Framework for Action regarding antimicrobial resistance and use; Ethiopia has a National Strategic Framework for Prevention and Containment of Antimicrobial resistance; and Sweden even boasts three such plans.
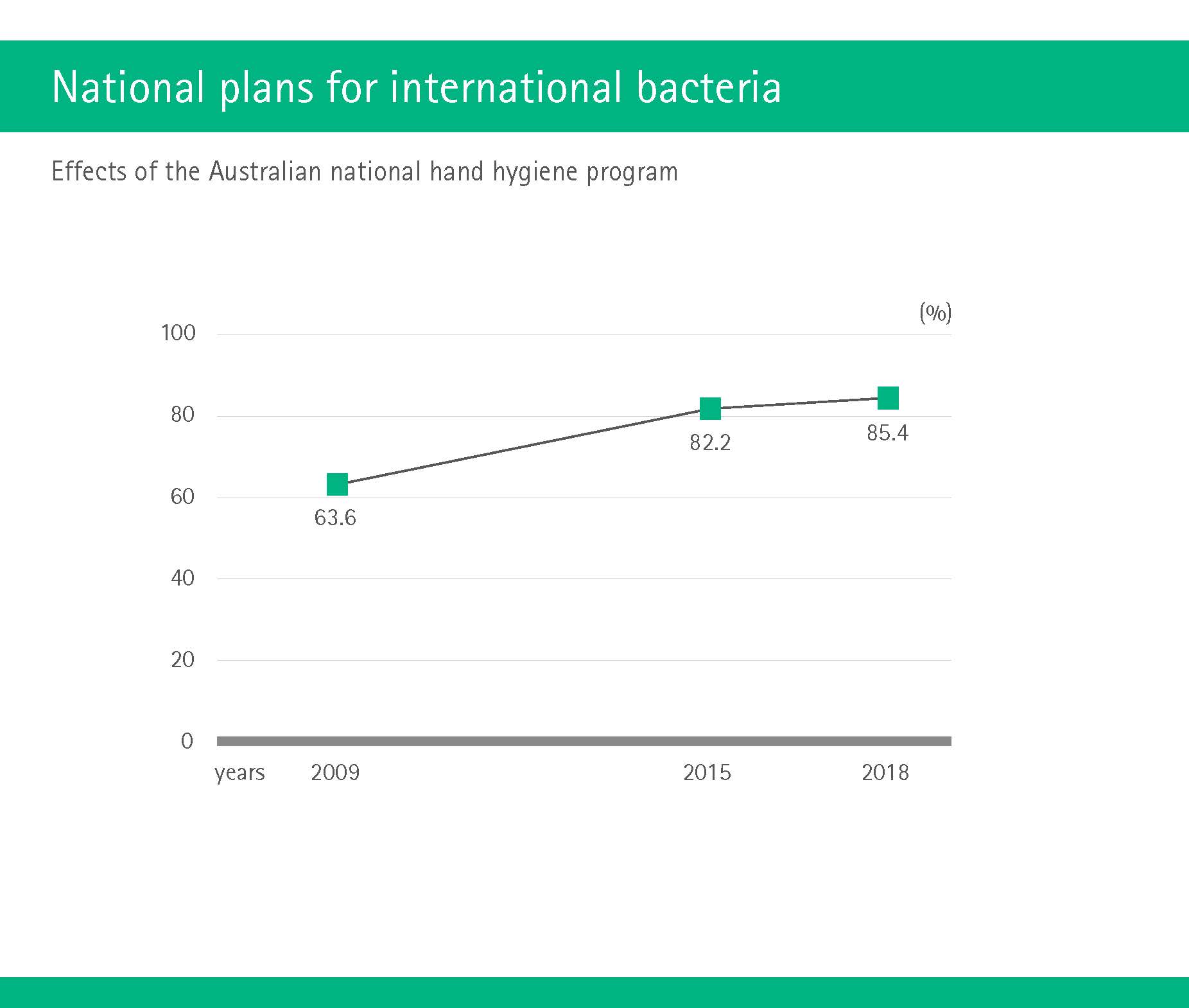
Australia, meanwhile, has taken on somewhat of an expert role in infection prevention. As early as 2009, the land down-under decided to kick off the world’s largest national hand hygiene program. Hospitals were obliged to undergo hygiene standards assessments as of 2013, and failure to meet these standards put hospitals at risk of losing funding and licensure. Unsurprisingly, there followed an increase of participating hospitals from 103 to 937 until 2017.
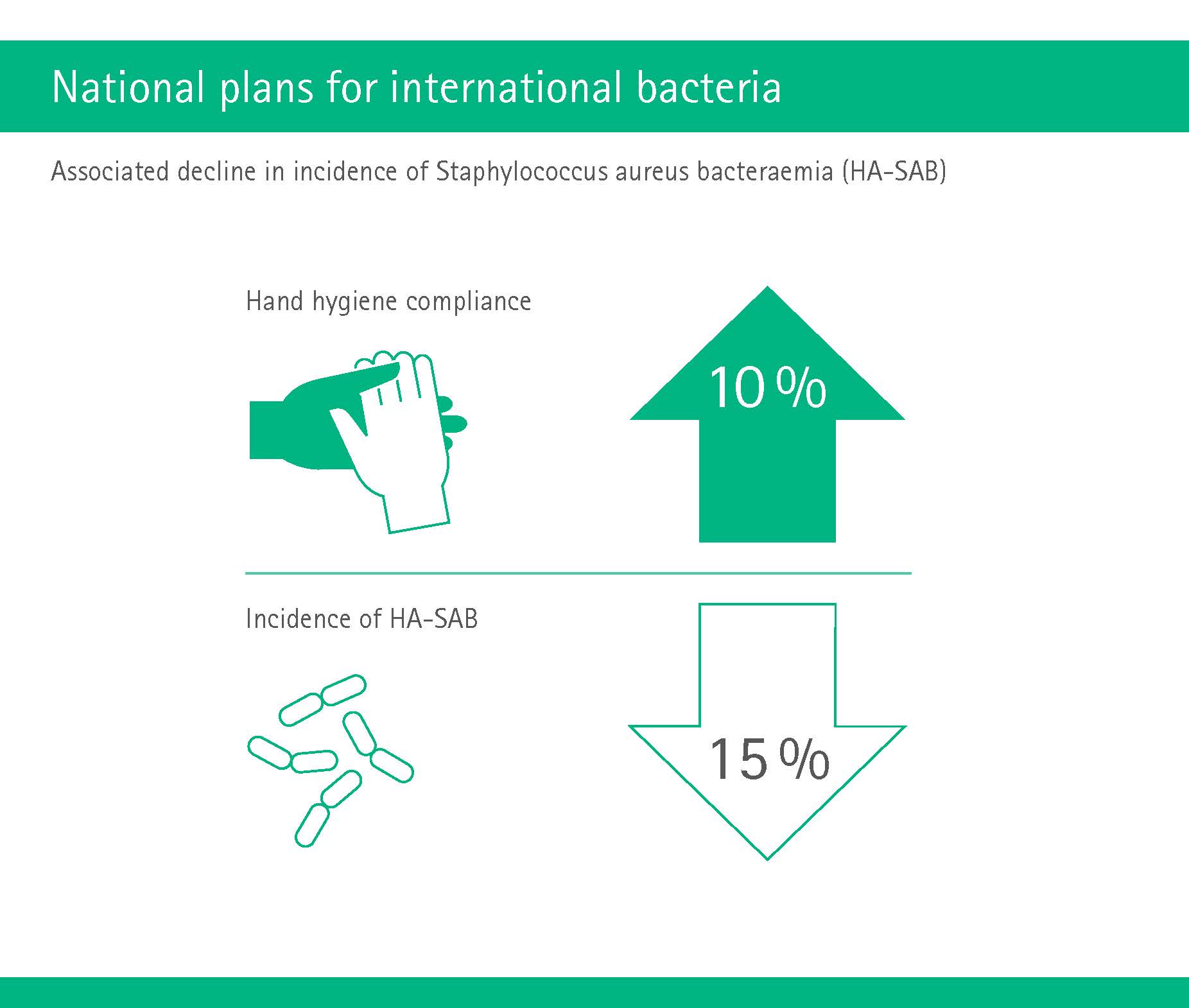
The success of the program consequently justified this approach, even if it was a somewhat forceful one: Hand hygiene compliance rates increased to a nationwide average of 85 percent. Crucially, it was also proven to reduce infections caused by the infamous Methicillin-resistant Staphylococcus aureus (MRSA). In 2018, the program’s experts published findings showing a significant association between improvements in hand hygiene compliance and declining healthcare-associated infections in the Lancet (Grayson ML et al, Lancet Infect Dis 2018;18:1269-1277).
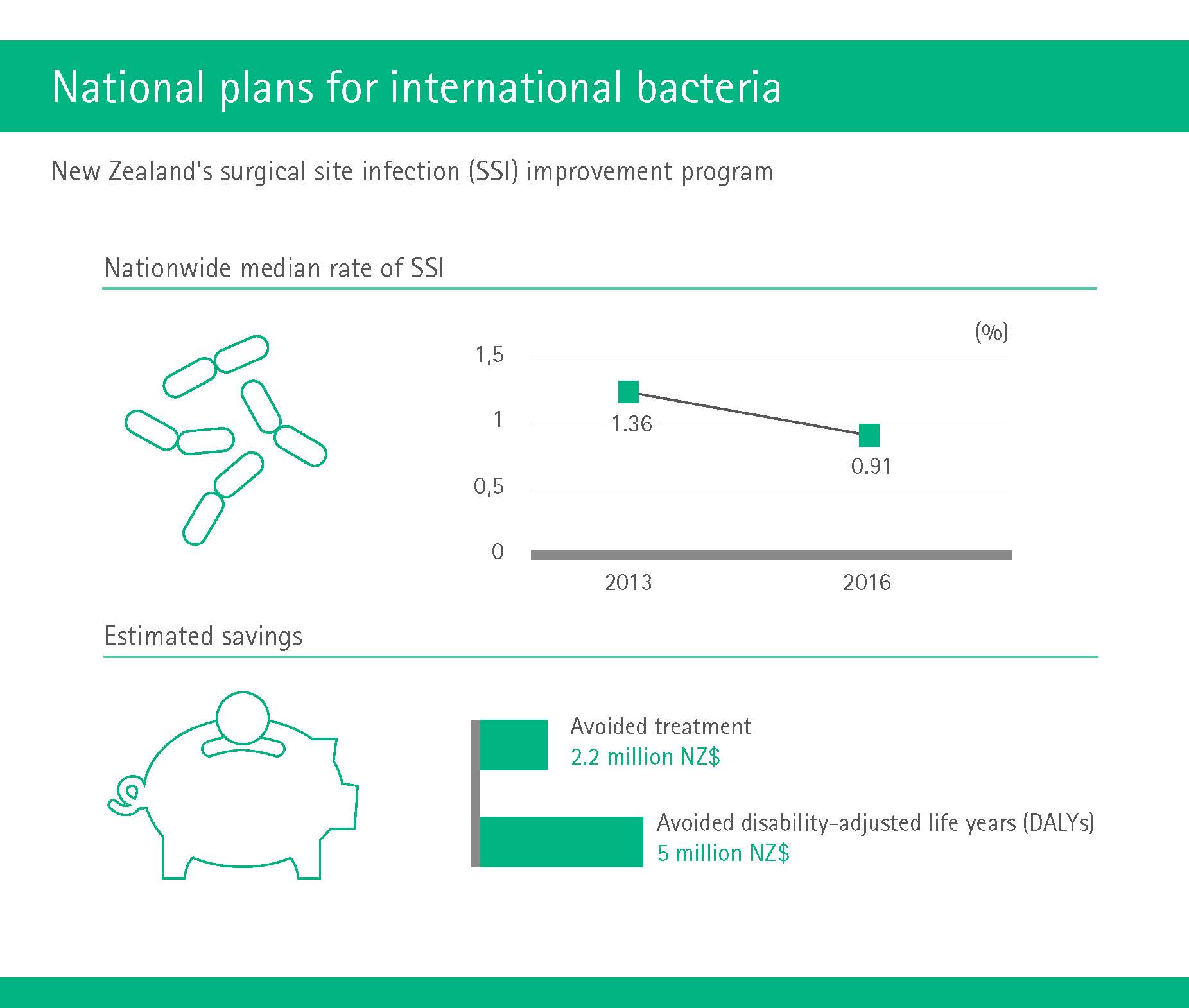
Aiming to reduce the incidence of Surgical Site Infections (SSIs), Australia’s neighbor New Zealand in 2013 introduced a national program that focused on i) surveillance, ii) compliance with evidence-based practices and iii) public reporting on changed practices and outcome data. By the end of 2016, the nationwide median rate of SSI had fallen from 1.36 percent to 0.91 percent. This equates to approximate savings of 2.2 million New Zealand Dollar (NZD) in avoided treatment, and avoided disability-adjusted life years (DALYs) of 5 million NZD (https://www.ncbi.nlm.nih.gov/pubmed/30048432).
And speaking of money, the United States in 2012 chose a completely different approach to infection prevention by establishing the “Hospital Readmissions Reduction Program” (HRRP) which stipulates reduced payments to hospitals for excess readmissions. Put simply, a hospital that has to readmit patients within 30 days is considered to not have done a proper job of keeping the patient healthy. Infections are important in this respect, because they are a major cause why patients need to go back to hospital.
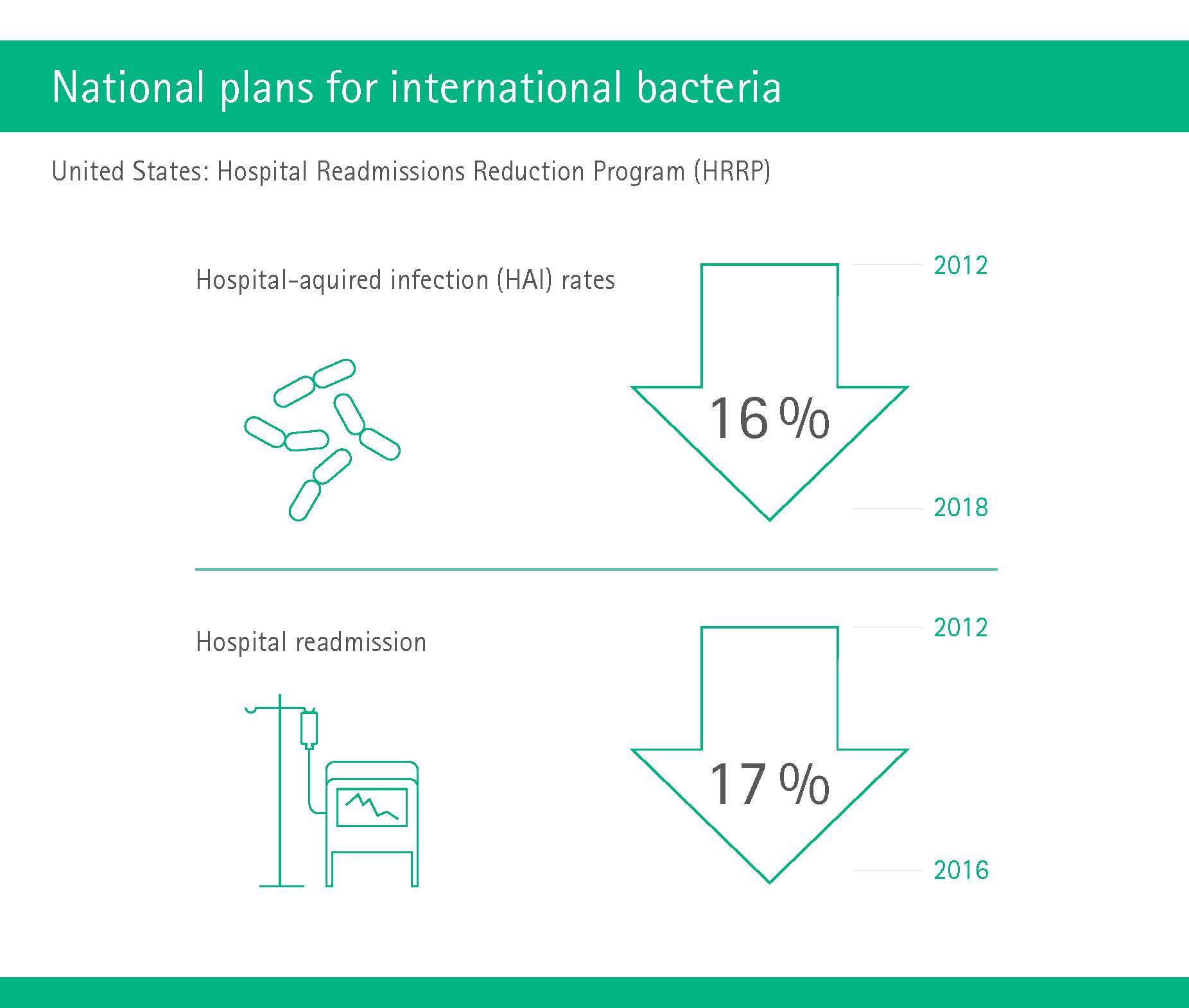
The program has delivered promising results. According to one paper from 2018, hospital-acquired infection rates went down by 16 percent since the introduction of HRRP (Magill SS et al, NEJM 2018;379:1732-1744). Another report showed a 17 percent decrease in hospital re-admission until 2016 (http://medpac.gov/docs/default-source/default-document-library/readmissions-january-2018-public9bd311adfa9c665e80adff00009edf9c.pdf?sfvrsn=0). Also, because sepsis is in fact the leading cause of hospital readmission (Mayr FB et al, JAMA 2016; doi:10.1001/jama.2016.20468), researchers called for this condition to be added to the program – but so far without success.
Finally, the United Kingdom in 2014 set out to position itself as the global leader in the battle against infections resistant to antibiotic drugs. In the following two years a commission led by economist and member of the House of Lords, Jim O’Neill, gathered information and proposed solutions from an economic and social perspective. In their final report, the Review on Antimicrobial Resistance (AMR) proposed recommendations to reduce demand for antimicrobials and in particular antibiotics on ten fronts, with the usual suspects public awareness, sanitation and hygiene as well as antibiotics in agriculture and the environment high on the list.
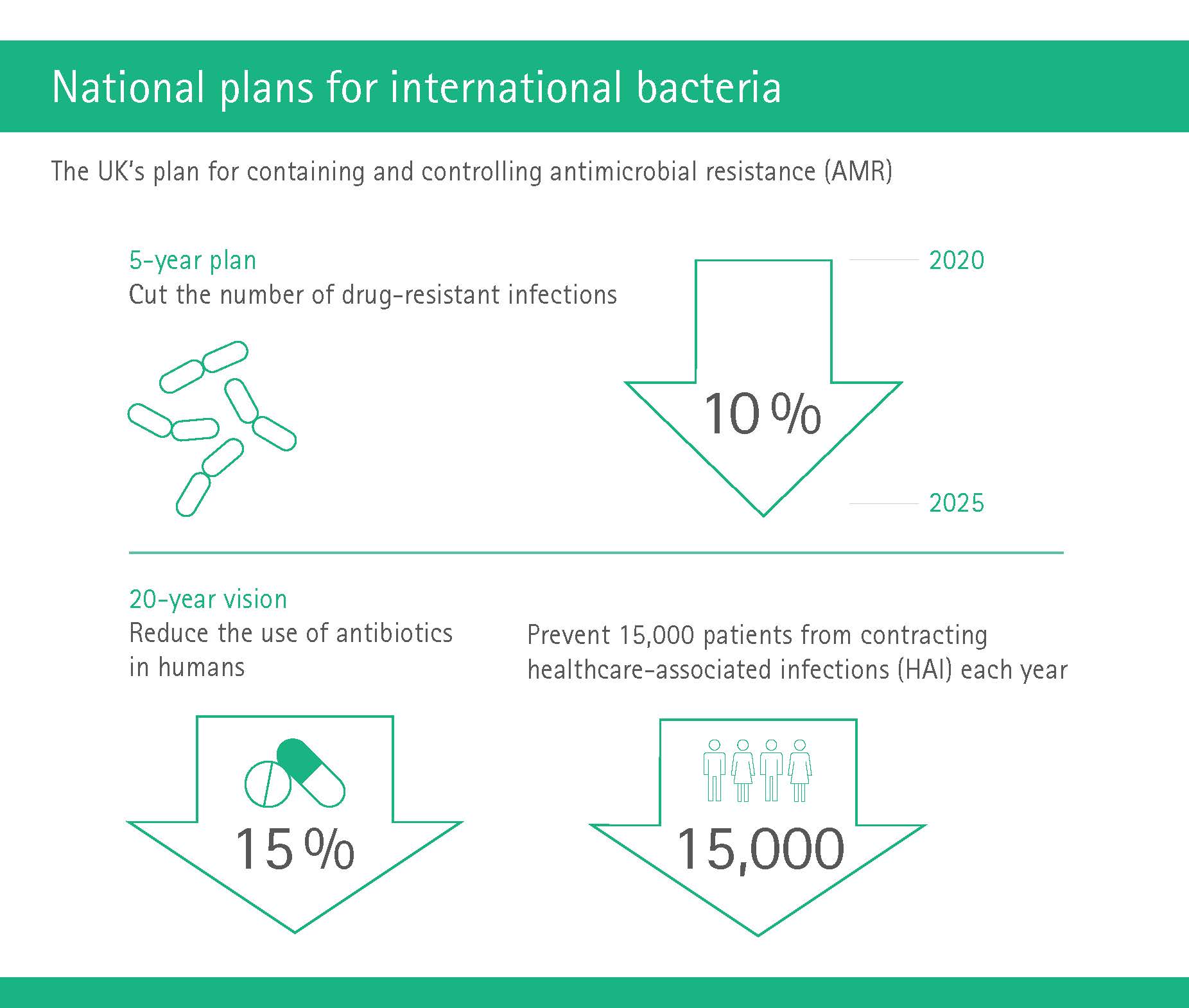
In January 2019, the UK government published a 5-year national action plan and a 20-year vision for how the UK will contribute to containing and controlling antimicrobial resistance by 2040. The plans include targets such as cutting the number of drug-resistant infections by 10 percent by 2025, reducing the use of antibiotics in humans by 15 percent, and preventing at least 15,000 patients from contracting infections as a result of their healthcare each year by 2024.
The transnational approach: Europe joins forces in public-private partnership
In Europe, the Enable project within the excellently named “New Drugs for Bad Bugs” program is working on developing potential antibiotics against specific bacteria. These bad bug scientists have already found new ways to target drug-resistant bacteria, convinced a pharmaceutical company to join them and recently selected their first antibiotic drug candidate (https://www.imi.europa.eu/projects-results/project-factsheets/enable).
Enable comprises more than 40 European partners from academia and industry who have joined forces in a six-year project funded by the Innovative Medicines Initiative (IMI) to develop novel antibiotics against the key “gram-negative” bacteria (these are considered more dangerous than their “gram-positive” cousins, as they often hide their outer membrane by a capsule or slime layer, which acts as “camouflage” against drugs). Enable was launched in 2014 and will run until 2020.
The IMI in turn is an EU public-private partnership funding health research and innovation, which boasts a budget of 5.3 billion Euros. Recently, the project selected a new antibiotic called apramycin as a candidate for clinical studies. Researchers at the University of Zurich were already able to demonstrate the efficacy and safety of this drug in animal models for various infections, including infections caused by some of the more dangerous drug-resistant bacteria.
„So far a lot of research effort to tackle this problem has been around hospitals and reducing clinical prescribing, but we now know that the environment is likely to play a part in how resistance to antibiotics can evolve and spread.“
News from the agricultural industry
But all these efforts mentioned until now have focused solely on humans. However, as we know, the (over)use of antibiotics in agriculture, in particular in animal husbandry, is one of the main drivers of antibiotic resistance. So what’s going on over there?
The news is cautiously optimistic. As mentioned above, some countries are starting to train veterinary students in the importance of sound antibiotic use. The agriculture industry has also realized the urgent need to develop strategies to replace antibiotics for food-producing animals, in particular poultry and livestock. So far, two international symposia on “Alternatives to Antibiotics” have been held. Hundreds of experts – from academia, government, regulatory agencies and animal industries in more than 25 countries – met up to discuss management plans regarding the reduction of antibiotics in animal agriculture and the development of alternatives to the all-important antibiotic growth promoters (AGP).
Here, phytochemicals come into play. Also known as phytobiotics or phytogenics, these are natural bioactive compounds derived from plants. In recent years, phytochemicals including common herbs and spices (thyme, oregano, ginger, cumin, coriander) have already been used in poultry for their potential as AGP alternatives. Essential oils have a demonstrable positive effect on body weight gain in broilers and also improve feed efficiency. A plethora of studies also demonstrated that extracts from plants such as dandelion or mustard improve the innate immunity in poultry and pigs. (https://veterinaryresearch.biomedcentral.com/articles/10.1186/s13567-018-0562-66)
Cranking up the heat on waste materials
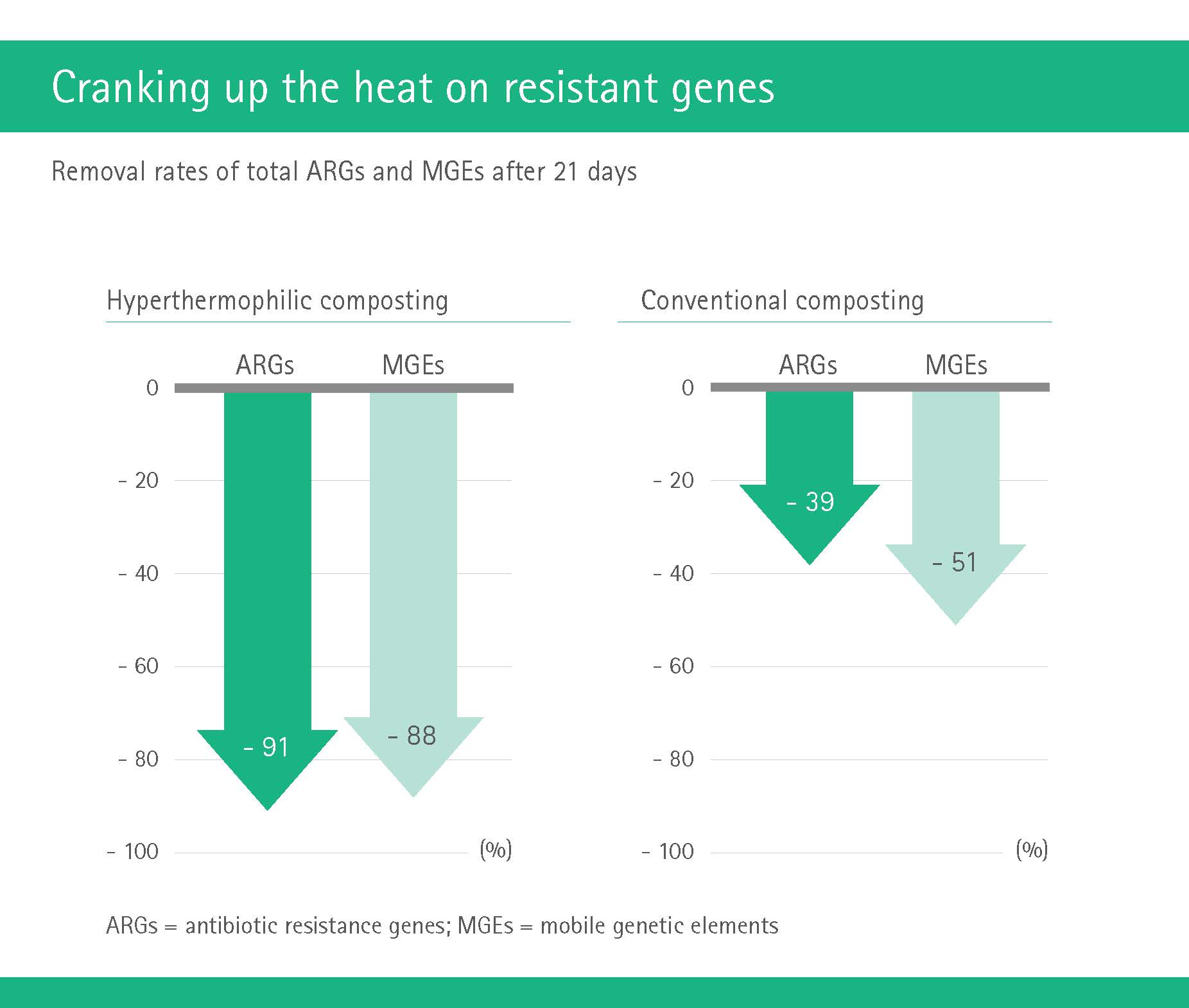
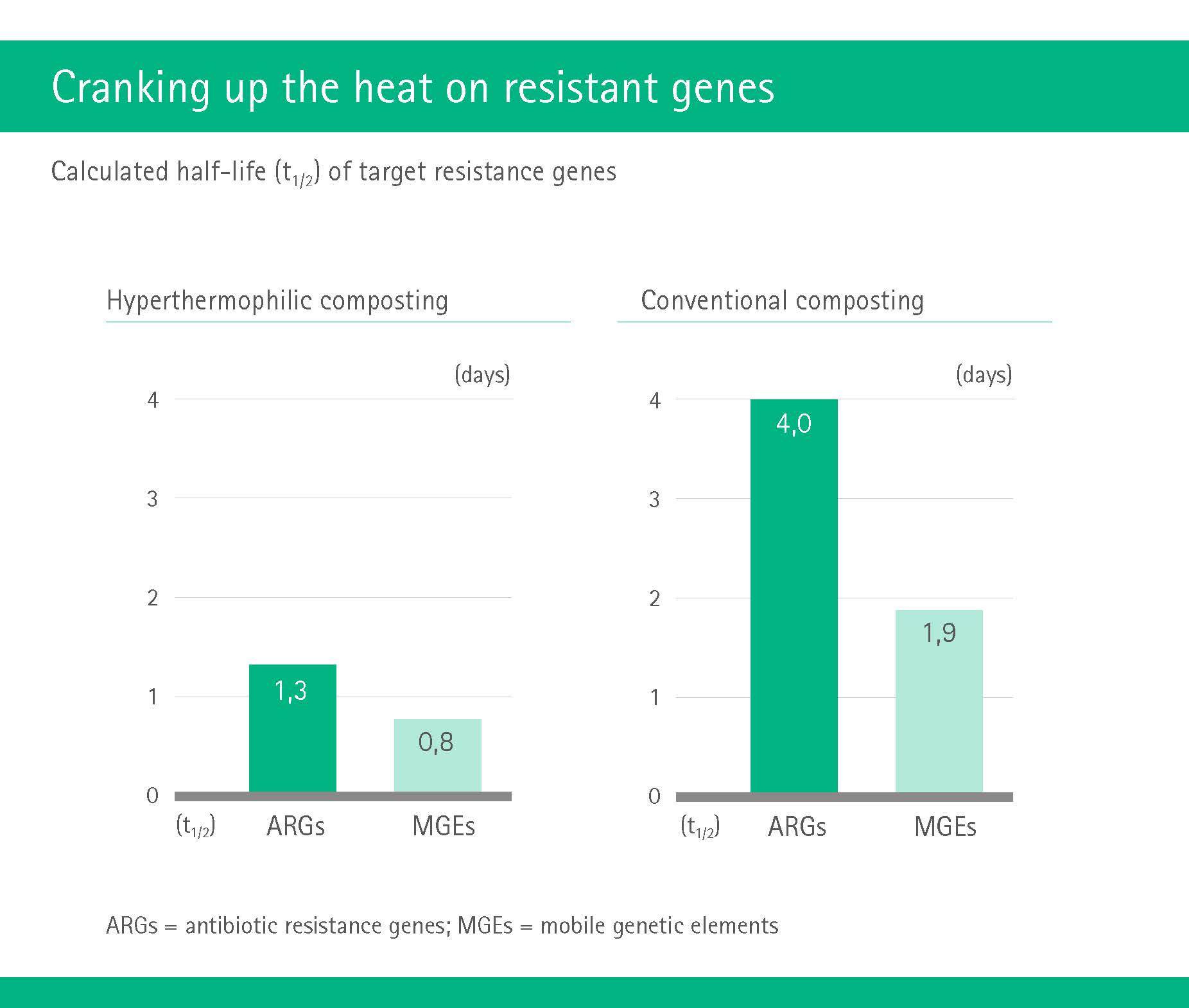
An international team of researchers hailing from universities in China, the United Kingdom and the Netherlands focused on one of the main transmission routes of antibiotic resistance: industrial compost. A mix of plant and animal waste, compost such as manure often contains resistance-carrying bacteria that have been transferred via excretion from animals which have been treated with antibiotics. When the manure is then reapplied in the soil to fertilize crops, the resistant genes are spread right alongside.
The researchers studied different composting methods and were particularly interested in the often present antibiotic resistance genes (ARGs) and so-called mobile genetic elements (MGEs) which play a key role in the spread of resistance. Comparing conventional composting to the method of hyperthermophilic composting which, very simply put, uses higher temperatures, the researchers found the latter method to be more efficient at removing both ARGs and MGEs than conventional composting. Hyperthermophilic composting, the study concludes, “thus represents a promising biotechnology for reducing the abundance of ARGs before solid waste land application”. (https://www.researchgate.net/publication/321502958_Hyperthermophilic_Composting_Accelerates_
the_Removal_of_Antibiotic_Resistance_Genes_and_Mobile_Genetic_Elements_in_Sewage_Sludge)
Among the number of recent studies and reports that have stressed the importance of the environment in spreading resistance to antibiotics, several have also focused on waste water. Swedish researchers, in a study published in early 2018, showed that even low concentrations of antibiotics can lead to high levels of resistance in bacteria which only exacerbates the pending antibiotic crisis since these low concentrations can now be found in many, if not most watercourses and lakes (https://phys.org/news/2018-04-antibiotic-resistance-small-amounts-antibiotics.html).
Shortly after, a study conducted at the University of Exeter Medical School confirmed that exposure to low concentrations of antibiotics in sewage waste water results in the same increase of resistant bacteria as at high clinical concentrations. The authors concluded that any water system that carries waste water run-off is a breeding ground for resistant bacteria and that the environment should thus be acknowledged as an equally important battleground in the fight against antibiotic resistance (https://phys.org/news/2018-07-environment-key-ground-tackle-antibiotic.html).
As you can see, there are no easy or straightforward answers to the global threat of antibiotic resistance. But governments, scientists and industry have to keep trying, searching and analyzing. As for the rest of us, we must all play our part as well, washing our hands, taking antibiotics only when necessary and demanding “free from antibiotics” animal products. Increased customer awareness of this sort plays a key role in pushing industry to develop alternatives. Otherwise, our alternative reality will be a return to the dark ages, where even a small scratch could kill you.





