Finding the cause first, then stage-appropriate treatment!
Far too often, chondral defects (defects of the cartilage) in the knee are treated by the numbers. Lasting treatment success can only be achieved by thoroughly researching the cause in conjunction with providing stage-appropriate, step-by-step treatment.
Please describe a typical patient with chondral defects in the knee!
Prof. Peter Angele: When talking about joint wear, most people think of older patients at least 60 years old who need an artificial knee. In my practice, however, there's a wide range of other patients with chondral defects requiring treatment. A typical patient I treat day to day is an ambulant patient around 32 years old whose knee cartilage has been damaged either by excess weight, improper mechanical stress or exercise. With these patients, it's especially important to do a differential evaluation and provide stage-appropriate treatment.
What are the most common chondral defects in the knee you see in your practice?
The most common would be degenerative arthrosis due to strain and wear. The second most common would be traumatic chondral defects, often related to sports injuries. Third would be chondral defects due to osteochondrosis dissecans. In this case, for reasons that aren't entirely understood, fragments of cartilage and bone become loose in the joint, restricting the mobility of the knee.
What needs to be kept in mind when diagnosing chondral defects in the knee?
Recognizing the extent of the chondral defect requires a precise clinical diagnostic of the knee joint. As a rule, an MRI examination is required for this. For determining concomitant injuries, an X-ray examination of the extended knee joint and a long leg standing X-ray are indicated. The goal of any clinical diagnostic should be determining the type, size, depth and area of the chondral defect in order to then be able to initiate the proper treatment. Despite the variety of instrumental diagnostic options, however, a clinical examination and an extensive medical history rank first: Is the patient overweight? Is the patient physically active? What caused the chondral defect? It doesn't help to treat a chondral defect if an underlying cruciate ligament rupture or a defective position - such as bowleggedness—isn't corrected.
Are there conservative treatment options for chondral defects in the knee?
There is no endogenous regenerative treatment option for arthrosis or chondral defects, the cartilage will not heal itself. That is, an intervention is always required to permanently remedy a chondral defect.
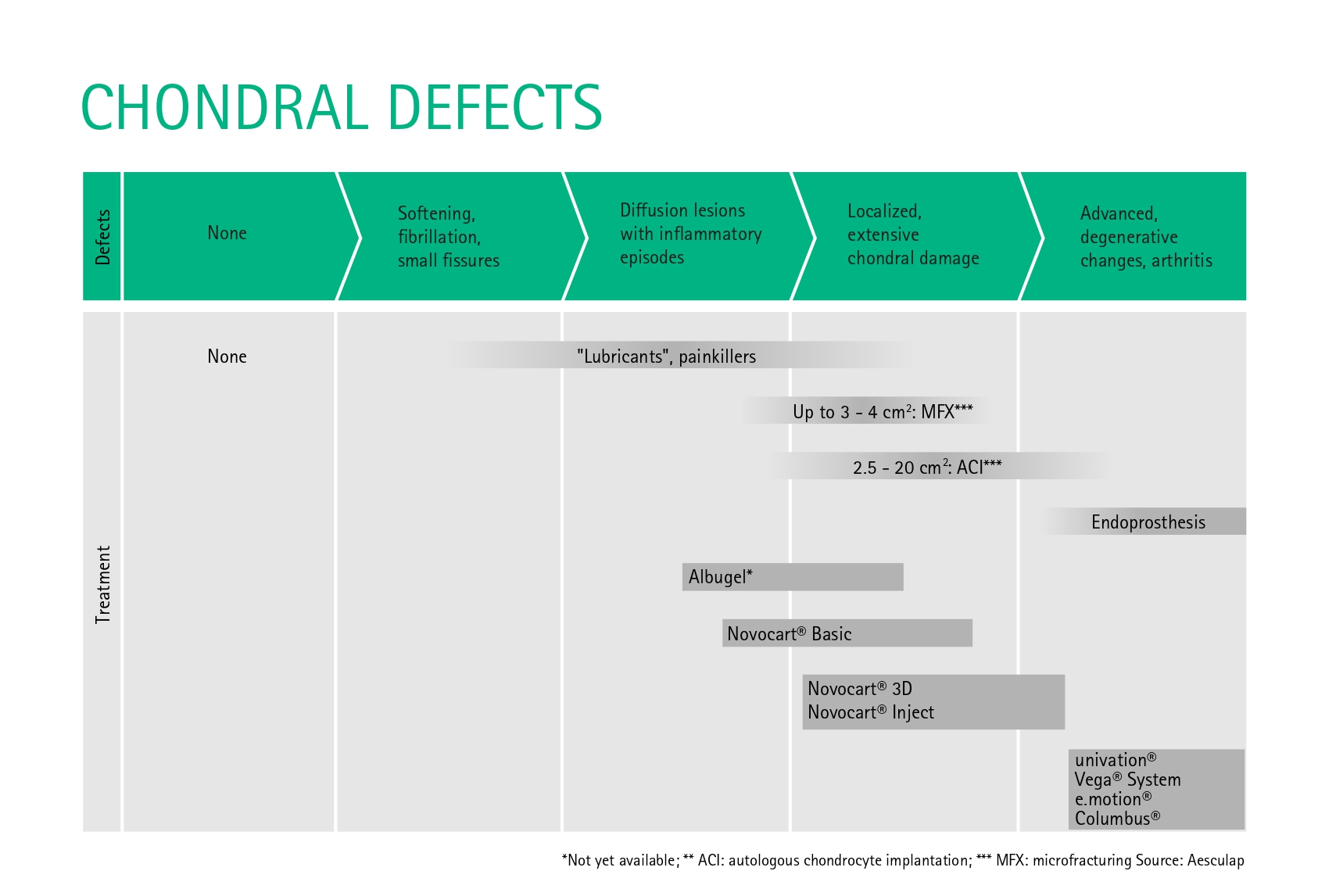
If, however, the chondral defect is in the early stage—minor fissures or diffuse lesions with the occasional inflammatory episode—the symptoms can initially be alleviated with a series of conservative measures. On the one hand, there are analgesics, hyaluronic acid injections and physical therapy. On the other, patients themselves can take steps toward their own improvement, such as by losing weight or adjusting their level of physical exertion. Of course, not all patients manage to slim down. And an ambitious athlete also won't agree to dial back their physical workload. This is where conservative treatment meets its limits.
What intervention is appropriate for smaller chondral lesions that no longer respond to conservative treatment?
The spectrum of conservative treatment is generally always exhausted when dealing with local, deep chondral defects that extend down to the bone. Depending on the depth and extent of the chondral defect, various treatment options are possible. For local defects up to 2 cm2, microfracturing in the affected area is recommended. In this procedure, small holes are drilled in the cartilage down through the subchondral bone plate, allowing stem cells from the marrow space to flow in. These stem cells cause new scar tissue to form, which fills in the chondral defect. This biological reconstruction can be assisted, if necessary, by introducing a biphasic, three-dimensional, collagen-based matrix (NOVOCART® Basic).
And how are more serious chondral defects extending over 2 cm² treated?
If the size is over 2 cm², an autologous chondrocyte implantation (ACI) should be applied. This is where several small samples of cartilage from less load-bearing areas are taken during an initial outpatient procedure, during which the joint is also inspected and the defect documented. These cartilage samples are then sent to the lab, where a biphasic, three-dimensional, collagen-based matrix is used to isolate and cultivate chondral cells over a period of four weeks. The autologous chondral cells produced in this manner (NOVOCART® 3D) are then implanted into the chondral defect in a second procedure. This second surgery should be an inpatient procedure. The success rate of this procedure is very high: The implant fails in just around six percent of cases, because it doesn't integrate or it comes loose. However, with major defects under the patella, the failure rate can be as high as 25 percent.
Minor osteochondral defects in the knee can be treated by osteochondral transplantation. This is where one or two osteochondral samples are taken from the periphery of the joint and transplanted into the chondral defect. With this method, however, the size of the defect is limited, since otherwise the sampling point can cause the patient other complaints. In general, an ACI is a suitable treatment for major osteochondral defects, such as osteochondrosis dissecans, as long as the chondral defect was filled in first. Patients with osteochondrosis dissecans have a very good prognosis.
What in particular should be kept in mind with an ACI?
The chondral defect needs to be clearly defined. It needs to be surrounded by healthy articular cartilage for it to be suitable for an ACI. Extensive cartilage loss, as seen in arthrosis, isn't suitable. I also make sure the causes of the chondral defect are included in the treatment regimen. Only then can chondral treatment be successful.
Lastly, it comes down to proper follow-up care. Weight shouldn't be put on the implanted area for several weeks in order not to jeopardize the production of chondral tissue by the implanted chondrocytes.
Do you get the impression that a chondrocyte implantation is often decided on too quickly in the field of chondral treatment?
It's more the opposite. These days, even the majority of larger chondral defects are unfortunately treated with microfracturing because it's a simple and easily controlled procedure. However, microfracturing is only suitable for defects with a limited extent. For larger chondral lesions, you shouldn't start out by trying microfracturing, rather you should go right for an ACI, which simply has a better chance of success in these cases. Less isn't always more!
How do the outpatient and inpatient sectors cooperate when it comes to chondral defects in the knee?
In our facilities, we can seamlessly provide all types of care, from outpatient to inpatient treatment, to inpatient treatment at our university hospital. This also allows us to adequately care for high-risk patients.
In other orthopedic practices and hospital departments, other ways to collaborate need to be found depending on the infrastructure and equipment of each facility.
However, in general it can be said that conservative treatment, along with pre-op and post-op care, is the domain of outpatient medicine. Microfracturing of small chondral defects can even be an outpatient procedure.
An ACI, on the other hand, should continue to be reserved for inpatient facilities. This question also doesn't even come up typically, because an ACI isn't even billable by a private practice, it's purely a DRG service.
By Antje Thiel
Contact













