Pain is not inevitable
“Get your kicks on Route 66” hum Hinrich Brek and Dr. Karl-Heinz Gnutzmann still together, then Brek dozes off on the operating table of the Kronshagen outpatient surgery clinic.
Maybe the 64-year-old is now dreaming about the Rolling Stones’ good classical Rock and Roll and a tour with his Harley. However, the small pump that will ensure a uniform administration of painkiller to his right shoulder for 50 hours after the procedure is part of the modern pain management arsenal. Anesthesiologist Gnutzmann has been using the Easypump for almost ten years now.
“Something is rubbing into my shoulder. It really hurts,” said the passionate biker as late as this morning. He now hopes the operation will relieve his pain. Relatively quickly after being diagnosed with shoulder impingement syndrome, it was clear to him: “I want surgery” – but not only that: An acquaintance told Hinrich Brek his experience with the same procedure. “Everything went well, but when he was driven home in the evening after the outpatient surgery, he had severe pain.”
Hinrich Brek doesn’t want this to happen to him. In a previous consultation with Dr. Gnutzmann, he decided to remain one night in the outpatient clinic and allow an inserted pump to administer a painkiller. “Why should I suffer?” he thought, even if he has to pay the cost of the overnight stay himself as it is not covered by insurance.

Even when lying on the operating table, he chats a little with the anesthesiologist in northern German dialect about his “iron hog from Milwaukee” and falls asleep soon thereafter. “Some patients really dream about what we were talking about when the anesthesia is induced,” says the anesthesiologist while placing the tube for artificial respiration into his patient.
Meanwhile, Dr. Matthias Zimmermann, surgeon, trauma surgeon and orthopedist, has entered the OR. Together with anesthesia nurse Robert Krenz and OR nurse Nicole, he repositions the patient to the left side, his right arm hangs extended from this body. “Pure regional anesthesia is not enough in this case because the physical pull on the arm is so strong,” explains Gnutzmann, “and therefore the procedure is done under general anesthesia”. He had already started pain management before the operation with the “classic” painkiller ibuprofen, which he gave Brek in tablet form. “We always want to stay one step ahead of pain,” he explains. Novalgin is administered during the anesthesia. “This is quite easy to organize.”

In the meantime, the surgeon starts with the arthroscopic surgery of Hinrich Brek’s shoulder joint. The changes below the acromion can be recognized on the monitor above the operating table: thickened tissue, the edge of the scapula has rubbed off the tissue and destroyed it, inflaming the bursa. “A classical picture in 40- to 60-year-old patients with shoulder joint symptoms due to an impingement syndrome,” confirms Zimmermann while he removes excess and damaged tissue endoscopically. Nurse Nicole “flushes”, i.e. starts rinsing and suctioning tissue. The patient’s blood pressure increases briefly a little bit. The surgeon glances at the anesthesiologist and just says “Kalle”, and Karl-Heinz Gnutzmann regulates systolic blood pressure from 100 to 110. “That’s optimal to keep bleeding in check,” he explains.

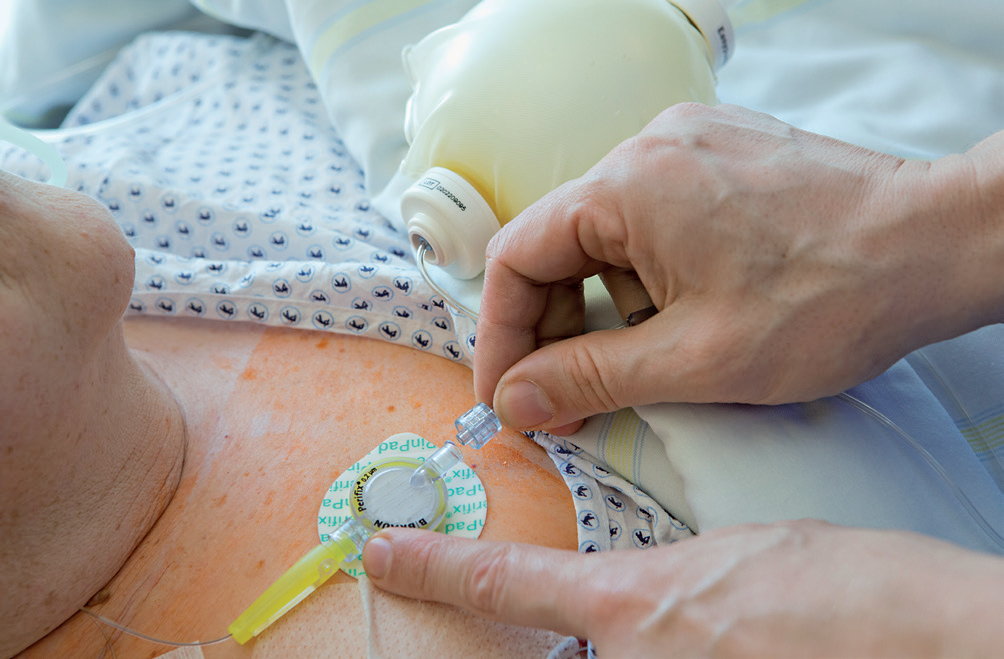
Meanwhile, the surgeon has ground down the clavicle bone so much that it stops rubbing. He sutures the insertion holes for the endoscopic instruments and leaves the OR after 40 minutes. Now it’s “Kalle’s” turn once again. While anesthesia nurse Robert monitors the emergence from anesthesia, Gnutzmann marks “landmarks” above the patient’s right scapula with a permanent marker. Finally, he introduces a 0.85-millimeter fine catheter into the upper supraspinatous fossa to a depth of about four centimeters. Then he adds approx. 30 milliliters of painkiller to the groove around the main nerve. He describes the advantage of block anesthesia: “The painkiller acts immediately and directly on the suprascapular nerve for the next four to six hours,” referring to the blockage of the nerve above the scapula. There is now enough time to lay the entry for the painkiller pump and fix it with transparent adhesive bandage.

“It’s good timing when the patient wakes up when we have finished placing the catheter,” explains Gnutzmann. Hinrich Brek mumbles, he is probably still rolling along Route 66. In the meantime, nurse Robert becomes sporty in the adjoining room: Two bags with 200 milliliters Ropivacain and a large 50-milliliter syringe are ready for filling the elastomeric balloon of the pain pump. He refills the syringe eight times and presses the liquid with some force into the Easypump, which takes a few minutes. The infusion device is now ready for use. About two hours after the procedure has ended, Hinrich Brek is cheerful once again. “Nothing hurts”, he notices relieved in the recovery room. Gnutzmann and nurse Robert close the Easypump’s supply line with one click in the catheter placed in the OR. The continuous supply of painkiller has been ensured. The control element regulates the flow through the skin temperature. Brek is already looking forward to a restful night up there on the ward of the outpatient surgery clinic. Maybe his dream trip across the U.S. will continue!












